Supporting long-term care and home care workers in the recovery from COVID-19
The outsized burden placed on continuing care workers by the pandemic has in many ways gotten heavier.
Executive summary
Manitoba experienced the tragic loss of over 700 residents in personal care homes due to COVID-19, resulting from some of the most severe outbreaks in long-term care homes across Canada. The tragedies inflicted by COVID-19 exposed the widening gaps in the Canadian healthcare system. Closing these gaps, in many cases, fell onto the backs of frontline healthcare workers forced to work under stress and staff shortages to ensure patient care. Since the outbreak of COVID-19 public attention has been drawn to the need to further support healthcare workers experiencing burnout, however relatively little attention in Manitoba has been focused on workers in long-term care and home care in recent months.
This report offers insight into the experiences of Manitoba continuing care1 staff working in home care and long-term care during the COVID-19 pandemic, drawing attention to issues around workload, staff shortages, workplace safety, pay and benefits both during the heights of the pandemic and afterwards. Results are based on a 2022 Probe Research survey of 1027 unionized, public long-term care and home care staff from Northern Manitoba (NRHA), Southern Manitoba (IERHA, PMH, and SH-SS), and Winnipeg (WRHA).
Results from this survey indicate that staffing within Manitoba’s public long-term care and home care programs has reached a breaking point. Persistent short staffing and increased overtime hours drive high levels of workplace stress leading to burnout amongst continuing care workers. Wages, which are below the provincial living wage in many cases, are insufficient for workers to save for their futures.
Dissatisfaction with benefits (time off, pensions, and extended health) contributes to negative physical and mental health outcomes. While many of these workplace issues existed prior to the outbreak of COVID-19, severe short staffing throughout the pandemic has intensified workplace stress and exacerbated understaffing. Over 50 percent of long-term care and home care staff who responded to our survey indicated that they are either very or somewhat likely to leave the profession in the next five years.
Our content is fiercely open source and we never paywall our website. The support of our community makes this possible.
Make a donation of $35 or more and receive The Monitor magazine for one full year and a donation receipt for the full amount of your gift.
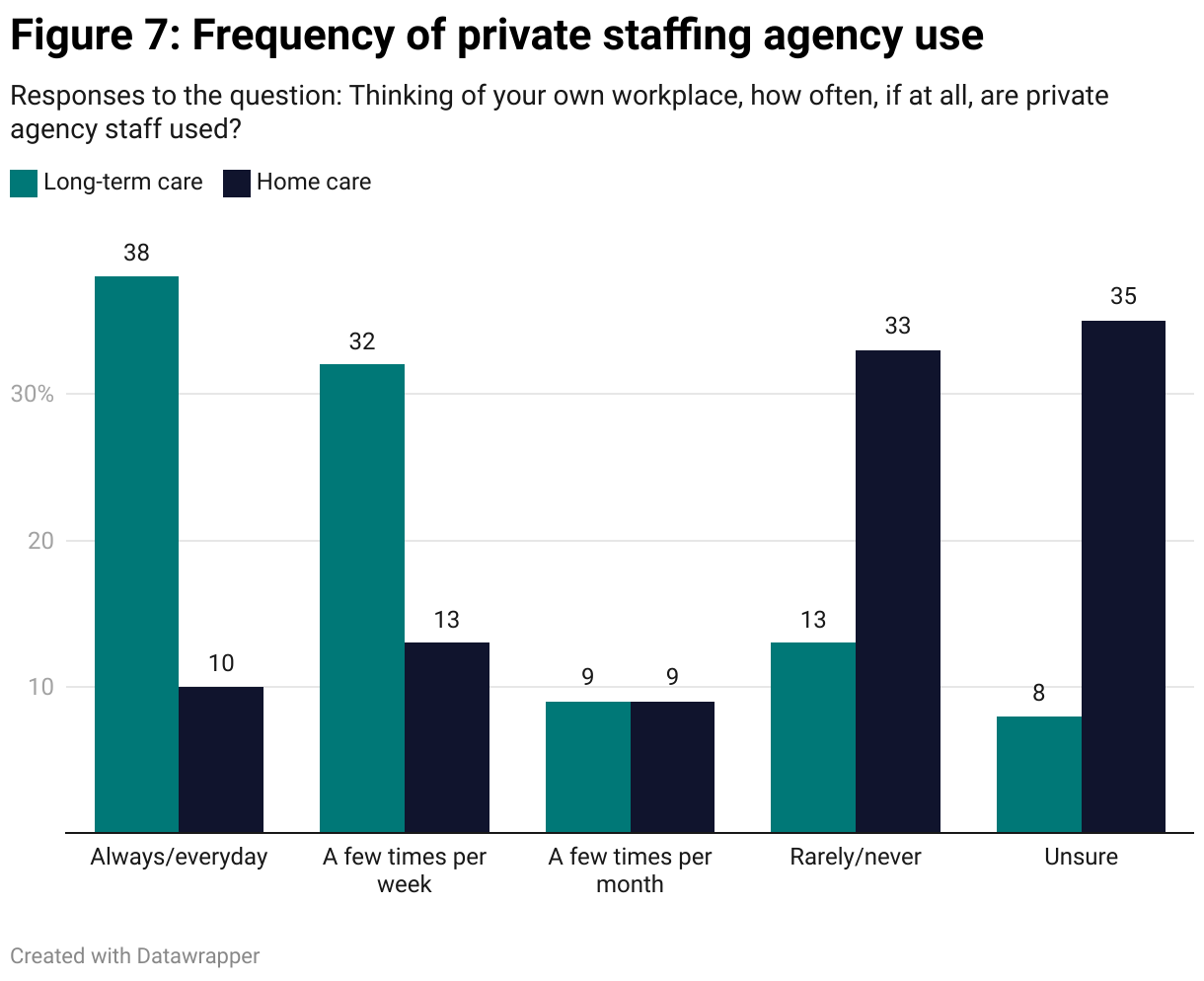
In response to staffing shortages in long-term care and home care, health authorities have turned to private healthcare staffing agencies to fill staffing gaps. Approximately 70 percent of long-term care workers surveyed reported working alongside private agency staff daily or a few times weekly. Staff across healthcare are increasingly moving to the private sector due to burnout, a lack of control over scheduling, and lower wages in the public sector. Filling gaps in the public healthcare workforce by contracting private agencies is a highly costly policy over the long term. Efforts should be made to recruit and retain continuing care staff in the public system.
As is the case across the country, women are overrepresented in Manitoba’s continuing care workforce, particularly racialized and newcomer women. These workers are particularly vulnerable due to workplace racism, which has increased since the onset of the pandemic, precarious immigration status, a higher likelihood to work under precarious employment relationships, and workplace harassment and violence (Nicholson and Hande 2023).
A just recovery from COVID-19 requires provincial governments to make the long-overdue investments necessary to repair our public long-term care and home care systems and build capacity for the future. Ensuring adequate staffing levels is a key element to ensuring patient rights to adequate care and reducing workload stress on staff. Further efforts should be made, including improving wages, benefits, and full-time hours, to ensure decent working conditions for frontline care workers.
The 2023/24 windfall in provincial revenues, including a large increase in federal health transfers, has rendered these investments easily achievable. Increasing staffing levels in Manitoba’s long-term care and home care programs to levels that ensure high-quality care, safer working environments, and an increase in full-time hours would cost $180.8 million annually (author’s calculations). Through a reprioritization of spending away from tax cuts, an $180.8 million boost in annual spending on long-term care and home care is easily within reach.
Introduction
It is no secret that workers in continuing care, including home care and long-term care, faced some of the most difficult conditions working on the frontlines throughout the COVID-19 pandemic. As of July 2022, 43 percent of all COVID-19 related deaths in Canada occurred in long-term care homes, despite long-term care residents making up less than 1 percent of the national population (National Institute on Ageing 2023). Manitoba had among the most COVID-19 related deaths per capita in long-term care (Loreto 2020), with some of the worst outbreaks in the country reported at Parkview Place and Maples Long-Term Care Home, both owned by Ontario-based Revera Inc (May 2020).
Since the outbreak of COVID-19 healthcare experts have repeatedly raised alarm over extreme levels of burnout among healthcare workers, leading to waves of resignations and early retirements, creating shortages of healthcare staff (House of Commons Standing Committee on Health 2023). In Manitoba, reports have noted shortages of over 350 doctors and a province wide vacancy rate of over 20 percent for nurses, exacerbated by COVID-19 related burnout in both instances (Doctors Manitoba 2022; Manitoba Nurses Union 2022). A report commissioned by the Manitoba government, tabled in the legislature by the opposition NDP in April 2023, found that over half of healthcare workers are looking for a new job due to burnout (CBC 2023). Staff cited excessive workloads due to chronic staff shortages, and a lack of control over shifts as primary reasons for seeking opportunities outside their current roles. However, while much attention has been focused on burnout among nurses and physicians, less attention has been paid to the experiences of continuing care staff working in home care and long-term care.
News coverage on continuing care workers, particularly in long-term care facilities, working in unsafe conditions for low-pay consistently featured in mainstream outlets during the first few months of the pandemic. The Maples Personal Care Home in Winnipeg became a high-profile example when eight residents died over a 48-hour period, forcing the health authority to call in assistance from paramedics and the Red Cross (Bergen 2020). The tragedy at Maples Personal Care Home resulted in the Stevenson Review of Manitoba Personal Care Homes (PCHs), which found that homes were unable to cope when pre-existing staffing shortages were exacerbated by illness-related absences. In line with trends across the country, deaths per bed were highest at for-profit PCHs where precarious staffing practices were more common (Annable et al. 2021). This was an important moment to reiterate the point repeatedly made by long-term care researcher Pat Armstrong: when it comes to patient wellbeing, the conditions of work are the conditions of care (Armstrong et al. 2020).
The systemic vulnerabilities within Manitoba’s long-term care and home-care systems did not begin with the pandemic. Under-funding of these two sections of the healthcare system has hit hard amidst an era of growing demands for care due to population aging and growing use of home care for outpatient care. Previous reports on long-term care and home care have noted a lack of adequate staffing as chronic vulnerabilities in these programs (CUPE 2015; Toews 2016). At the same time, these two sectors have consistently been used as testing grounds for privatization agendas which have resulted in mismanagement and service reduction (Shapiro 1997; Silver, Scarth, and Shaw 1997; Baines 2021; Cohen and Armstrong 2023).
As with other sectors and occupations that were highly exposed to the effects of COVID-19, the care sector is disproportionately staffed by women, racialized workers, and newcomers. These workers were hit hardest by employment and income losses during the COVID-19 recession, and are still struggling with higher than average employment and income losses (Scott 2022a).
In response to Manitoba’s healthcare staffing crisis, the provincial government launched its $200 million Health Human Resources Action Plan in November 2022. Billed as a comprehensive strategy to retain, train, and recruit healthcare professionals, the plan makes little mention of staff within Manitoba’s long-term care and home care programs, despite clear need for a staffing plan within these sectors of healthcare. In particular, the strategy makes no mention of strategies to recruit and retain Health Care Aides (HCAs) and Home Support Workers (HSWs) who provide the majority of direct care in Manitoba’s continuing care system. The results of the survey outlined below should be instructive for a provincial strategy to recruit and retain staff in home care and long-term care, repair relationships with staff, and improve quality of care for residents and clients.
Long-term care and home care in Manitoba
Long-term care
In Manitoba, long-term care is provided through 125 personal care homes (PCHs) situated throughout the Province. PCHs are owned and operated through a mix of public, private (for-profit), and non-profit models. 19 of Manitoba’s 125 PCHs are privately owned, however since these facilities are larger in size, for-profit care homes operate 25 percent of beds in the province. For-profit care homes are concentrated in Winnipeg and Brandon where they make up 40 percent of facilities (Armstrong et al. 2019). Public PCHs are situated throughout the province in rural communities and connected to larger healthcare facilities in larger urban centers. Non-profit PCHs have been a longstanding part of Manitoba’s long-term care system, with ownership and operation of these homes typically undertaken by religious and philanthropic organizations. Almost all staff across public, private (for-profit), and non-profit PCHs are unionized.
Operation and maintenance costs of PCHs are mostly covered through provincial grants distributed to regional health authorities (RHAs), however partial costs are covered through means tested resident fees. Private, for-profit PCHs receive the same funding grants as public facilities, and resident fees are capped to match rates at public and non-profit facilities. Daily resident fees in Manitoba PCHs range from $39.90 to $96.40, depending on income (Government of Manitoba 2023a).
Care work at PCHs is done by doctors, direct care nurses (RNs, RPNs and LPNs), health-care aides (HCAs) and other direct care professionals, alongside facilities and maintenance staff. The majority of care hours per resident are provided by HCAs and other direct care staff.
Women make up the vast majority of workers in PCHs. Results from our survey indicate that over 85 percent of long-term care staff in Manitoba personal care homes identify as women. A large and increasing proportion of workers in PCHs are racialized women or newcomers. Previous studies in Manitoba estimate that 70 percent of workers in Manitoba PCHs were born outside of Canada (El-Bialy et al. 2022).
Home care
In 1974, Manitoba became the first province in Canada to introduce a province-wide home care program. Home care programming, or what was then termed community care, was born out of a desire to invest in preventative medicine, reduce reliance on hospitals and personal care homes, and to respond to the needs of an aging population (Shapiro 1997).
Home care workers provide core services including personal care, nursing, occupational and physical therapy, household maintenance, meal preparation, laundry, and respite (Toews 2016). According to data from the Winnipeg Regional Health Authorities home care program, health care aides (HCAs) and home support workers (HSWs) perform over 80 percent of service hours, with the remainder performed by nurses and other allied health professionals (ibid). Similar to long-term care, most work in home care is done by women, many of whom are racialized or newcomers. Our survey indicates that over 90 percent of home care workers identify as women, even higher than long-term care staff in personal care homes.
Across the country, home care services are delivered through a mix of private and public service delivery models. Home care services in Manitoba are primarily provided by the public sector (Marier 2021). Per-capita public spending on home care is generally substantially higher in Manitoba than in other provinces (ibid). From 2015 to 2019, per capita public spending on home care was $305 per year compared to a Canadian average of $260 per year (Nicholson and Hande 2023:10).
Public home care services include both home care performed by Regional Health Authority (RHA) staff as well as self and family managed care. Public home care is provided on a universal basis with a goal to delay or prevent the need for institutionalized care. As of 2016, there were approximately 3500 full-time equivalent home care staff employed by RHAs across the province, all of whom are unionized (Toews 2016). This includes nurses, HCAs, HSWs, and administrative staff. Under self and family managed care, clients are provided with funds to hire and manage their own home care arrangements. No data is available on the number of home care workers employed under self and family managed care arrangements.
Despite higher public spending on home care in Manitoba, the supply of home care services is unable to meet demand. This is leading to growing demand for private and non-profit home care services, which offer clients with greater flexibility over scheduling (ibid). These services are only available to those with the means to pay out of pocket. Work in private and non-profit home care agencies is unregulated, and workers are not unionized.
The conditions of work are the conditions of care
Research from across North America has consistently reinforced the positive relationship between higher staffing levels and patient outcomes in long-term care and home care (Collier and Harrington 2008, Jansen 2011, Boscart et al. 2018). Clients in more highly staffed long-term care homes tend to be at lower risk of weight loss, spend less time in bed, experience higher levels of social engagement and are less likely to be hospitalized (CUPE 2015, Armstrong and Cohen 2023). A large study conducted by the United States Centre for Medicare and Medicaid on behalf of the US Congress ultimately found that 4.1 hours of care per resident per day (HCPD) was the bare minimum required to ensure patient health and safety (Health Care Financing and Administration 2002). More recent research from the US finds that standards should be higher than 4.1 hours of direct care, recommending a range of daily care hours based on patient acuity from 4.3 hours to 6.8 hours per day (Harrington et al. 2020). The mix of staff between RNs, LPNs, health care aides, and others is important for patient care.
Canadian provinces vary considerably on standards for direct patient care hours. In response to dire conditions in Canadian long-term care homes during the pandemic, the federal government launched a review into standards in long-term care. The voluntary standards that emerged from the review fell short of requiring a certain number of care hours per day. Still, the Health Standards Organization, which conducted part of the review, found “evidence indicates that LTC home residents require a minimum of 4.1 hours of direct care per day. Higher staffing levels improve quality of care, especially as residents’ care needs become more complex.” (Health Standards Organization 2023: 38) Many patient advocates have called on provinces to adopt legislation governing minimum direct hours of care in long-term care homes (Roman 2023).
Manitoba’s Department of Seniors and Active Living has set targets for 3.8 paid daily hours of care in PCHs, however Manitoba does not currently have legislated standards for direct care hours and long-term care advocates question whether the 3.8 HCPD guideline is being met (Froese 2022a). This target places Manitoba ahead of many other provinces, but far behind Ontario and Nova Scotia who are set to require 4.0 and 4.1 daily paid hours of care in long-term care homes in the coming years (Arulnamby and Sinha 2023).
Care work, austerity and healthcare privatization in Manitoba
Underfunding and privatization are not new issues for Manitoba’s long-term care and home care programs. Since these two programs were brought into the provincial welfare state by the Schreyer government in the early 1970s, there have been several attempts to hand operation and ownership of Manitoba’s continuing care system over to the private sector (Twomey 2014).
Two decades after home care’s launch in 1974, provincial government plans to privatize the services were leaked to the public by the then opposition NDP. The public outcry that ensued culminated in a province-wide strike by home care workers in 1996, with the workforce demanding the government contract out no more than 10 percent of staffing. In the face of widespread opposition from home care workers and the public, the government went ahead with a two-year contract to privatize 10 percent of Winnipeg’s home care workforce, with the contract awarded to Olsten Corporation.
Claims that privatizing home care services would reduce government costs were quickly disproven by revelations of Olsten Corporation’s mismanagement of healthcare contracts in the US, including widespread malpractice and excessive CEO payouts (Silver 1997). Amid a wave of public opposition, the province was forced to abandon its privatization plans.
The Olsten debacle put home care privatization onto the back burner for two decades until, in 2017, amid another attempt to drastically cut healthcare spending, the Pallister government released plans to contract out home care services. A contract was signed with two Ontario corporations to supply healthcare aides and other support staff for the new “Priority Home” program.
As during the Olsten affair, the concern over private sector management of home care operations is that for-profit firms create ‘savings’ by pushing down wages, cutting staff, and squeezing hours for resident care, as well as time to provide clients emotional or social care (NUPGE 2019). Under a for-profit model, ‘savings’ generated by lean service are passed onto shareholders as profit.
Proponents of continuing care privatization argue that private firms increase competition and drive innovation in the sector. Across most Canadian provinces, including Manitoba, long wait lists for public long-term care and home care services and fixed per-client public funding mean there is little incentive to improve service (Armstrong et al. 2019). Large firms can afford to take an initial loss on home care contracts in the hope that they can eventually crowd out competitors and raise prices.
Ownership structures of for-profit long-term care homes have become increasingly financialized in recent years, with shares of large chains publicly traded on stock exchanges or owned by private equity firms and real estate investment trusts. In some circumstances owners subcontract operations within care homes, creating layers of profit-seeking. Under financialized ownership models, profit is the primary goal of owners, and in regions where land prices are high, care homes are often viewed as real estate investments (Brown, Arya, and Longhurst 2021).
Attempts to bring home care and long-term care operations under a private, for-profit model have emerged amid growing service demands. Since the launch of the home care program in the 1970s, both measures to reduce healthcare costs and the growing demands of an aging population have been placed on the shoulders of home care workers. The 2016 Future of Home Care Services in Manitoba report commissioned by the Province found that home care aides are increasingly dealing with higher acuity patients as hospitals seek to expedite patient discharge and reduce institutional care, both in an attempt to reduce costs (Toews 2016). The 2016 review was launched following revelations from Manitoba’s Auditor General that, at the time, Winnipeggers had to wait an average of 37 days to begin receiving home care services (CBC News 2015). Although the issue was brought into the public eye in 2016, the negative impact of provincial austerity measures on home care workers have been recognized since the 1990s (Jones 1996).
The Future of Home Care Services report recommended the province hire between 90 and 100 new home care staff per year over the next two decades to meet the needs of an aging population, however little has been done to attract and retain additional staff. The same report found that home care staff vacancy rates among regional health authorities have consistently sat around 8-10 percent (Toews 2016). Between 2017 and 2021, home care funding per client was reduced in most Manitoba regional health authorities despite growing demand (Da Silva 2022). Documents tabled in the legislature by the opposition NDP showed that Southern Health Region had a 24 percent vacancy rate for home care attendants between 2017 and 2021, leading to a growing waitlist for care (ibid). Similar documents from the previous year showed a 25 percent vacancy rate in the Prairie Mountain Health Region (LeTourneau 2020). In August 2022 health support workers from across the province, who had been working without a contract for over five years, agreed to a new deal that narrowly avoided a strike (Froese 2022b).
Experiences in long-term care homes during the pandemic made clear the deficiencies of private sector management of continuing care. For example, in Ontario deaths due to COVID-19 were far higher in for-profit homes than in non-profit facilities (Ferguson 2021). In April 2020 the military was called in to assist in long-term care homes struggling to provide adequate care, which culminated in a report detailing disturbing conditions within long-term care facilities, the majority of which were for-profit (CBC News 2020; Cohen and Armstrong 2023). These findings underline the previously known tendency for private long-term care facilities to operate facilities with fewer staff or other resources and to delay facility repairs, leading to negative outcomes such as higher rates of resident hospital transfers (Cohen and Armstrong 2023).
As in Ontario, for-profit long term care homes in Manitoba faced a public backlash during the pandemic due to severe outbreaks and high death rates in these facilities. COVID-19 outbreaks at The Maples Care Centre, owned by Revera Inc., were so severe that this home became the subject of the Stevenson inquiry, which found a lack of adequate staffing levels to be a critical issue for service quality (Government of Manitoba 2022a). Parkview Place, also owned by Revera Inc., received national attention for one of the province’s longest and deadliest outbreaks, leading to thirty deaths over four months (Brown, Arya, and Longhurst 2021).
Gender, race, immigration and characterizations of care work in Canadian healthcare
As care work scholar Donna Baines writes, “Care work is generally viewed as the natural activity of women with few boundaries on their assumed desire and capacity to provide care, regardless of pay or working conditions” (Baines 2021). Care work in Canada, whether in long-term care facilities, clinics or delivered through community-based services such as home care, has long been largely performed by women who have struggled against a lack of value attached to care labour. Poor funding and support for this care work relative to other sectors of healthcare reflects this perceived lack of value. Policy makers tend to represent care work as unskilled and disposable, diminishing the contribution of care work to overall healthcare. This gendered policy divide was highlighted in the 2006 Royal Commission on the Future of Health Care in Canada, which differentiated between ‘direct’ and ‘ancillary’ health care services, supporting a view that ‘ancillary’ care work has a different connection to healthcare and that while direct services were not apt for privatization, ancillary services could be safely privatized (Armstrong and Laxer 2006). These ancillary services include food preparation, cleaning, home-support, and secretarial or clerical work.
Care worker actions to increase wages and improve working conditions have often been met with public hostility, as connecting “pay with care is seen by many to turn it into a cold economic transaction rather than a warm, family-based, rewarding labour of love” (Baines 2021). The COVID-19 pandemic laid bare the hollow nature of these objections. Care work is a fundamental service which must be properly resourced to ensure the safety and dignity of staff and those receiving care. Wage top-ups for essential care workers were offered to care workers across provinces during the pandemic, recognizing the risk and importance of this work during a health crisis. Federal funding for wage top-ups was made available to provinces on a cost sharing basis, with provinces free to define the terms of top-ups. Manitoba rolled out its Caregiver Wage Support Program in November 2020, which offered a $5 wage top-up for hours worked between November 2020 and January 2021 (Government of Manitoba, 2021). Wage top-ups were only offered to workers earning less than $25 per hour. With payments averaging $850, this support was far below what was offered in other provinces (Scott 2021). Across all sectors, Manitoba spent $155 million on wage top-ups, leaving $10.5 million in federal funding on the table (ibid).
In Manitoba, home care staff were working without a contract throughout the pandemic, with the expired contract for these workers dating back to 2017. Home care staff were finally offered new contracts in August 2022, which delivered a total pay increase of 9.6 percent between 2017 and 2024, however the provincial government has been slow to implement contract provisions such as paid rest breaks and evening and night shift premiums (Froese 2022b; May 2023). A total pay increase of 9.6 percent will not prevent home care staff from experiencing real wage losses due to inflation, which peaked at 9.4 percent year-over-year in Manitoba during June 2022 (Statistics Canada 2022). Real wage losses for care workers in Manitoba are consistent with trends across Canada, where slow wage growth has been eating into care worker purchasing power (Scott 2022).
In addition to a highly gendered division of healthcare services acting upon care workers in Canada, care work tends to be racialized across provinces. Increasingly care work in Canada is provided by migrant workers, recent immigrants and refugees, many of whom are racialized women. Recent data from Manitoba PCHs estimates that 70 percent of workers were born outside Canada, and most work part-time or casually (El-Bialy et al. 2022). In response to staffing shortages, federal and provincial governments have adjusted their immigration policies to facilitate the entry of care workers into health and social care settings (Hande and Nourpanah 2022). As part of Manitoba’s Health Human Resources Action Plan, the Province is increasing nurse recruitment efforts in the Philippines. Such recruitment strategies have the potential to be transformative for health and social care, however documented issues with working conditions and immigration policy have resulted in low retention of immigrant health workers. Low pay and a lack of benefits, understaffing, labour casualization, and minimal settlement infrastructure undermine the retention of qualified staff (Nourpanah et al. 2018). Further, closed work permits and an arduous permanent residency process delay family reunification and contribute to dividing the workforce along lines of immigration status and racial hierarchies (Tungohan 2021).
Alongside the gendered and racialized nature of work within long-term care and home care, the shift to austerity and privatization within long-term care has broader gendered implications. One way governments privatize long-term care is by providing an inadequate number of long-term care beds (Armstrong et al. 2019). This lack of beds shifts the responsibility for care onto families, where care work again tends to be performed through women’s unpaid labour. Further, a lack of long-term care beds forces many to seek more expensive alternatives such as private assisted living facilities. Elderly women, who tend to have smaller lifetime savings in old age, can be forced into unaffordable care arrangements due to a lack of availability in the regulated public system.
Austerity and privatization agendas, as well as systemic gender and race-based inequities in healthcare funding, are placing increasing pressure on care workers. The harsh working conditions created by this underfunding ultimately compromise the quality of care available through long-term care and home care programs across the country. To build a care sector that can look after clients with compassion and dignity and prepare for increasing demands on this sector of healthcare, policymakers must adequately fund public long-term care and home care programs.
Survey results
To create a portrait of current working conditions in Manitoba’s home care and long-term care sectors, the Canadian Centre for Policy Alternatives Manitoba office contracted Probe Research to survey unionized long-term care and home care staff in Manitoba’s public system. In July 2022, 1027 home care and long-term care staff were electronically surveyed to understand working conditions within these two sectors after two difficult pandemic years. The survey was distributed with the two unions representing home care and long-term care workers in Manitoba: Canadian Union of Public Employees (CUPE) and the Manitoba Government Employees Union (MGEU), using union communication channels to gather responses. Respondents were asked a series of questions covering workplace demographics and employment characteristics (including pay, hours, tenure), staffing levels, health and safety at work, effects of working during the pandemic, and the future of their work. Responses were collated and analyzed by Probe Research.
Who works in Manitoba’s care sector?
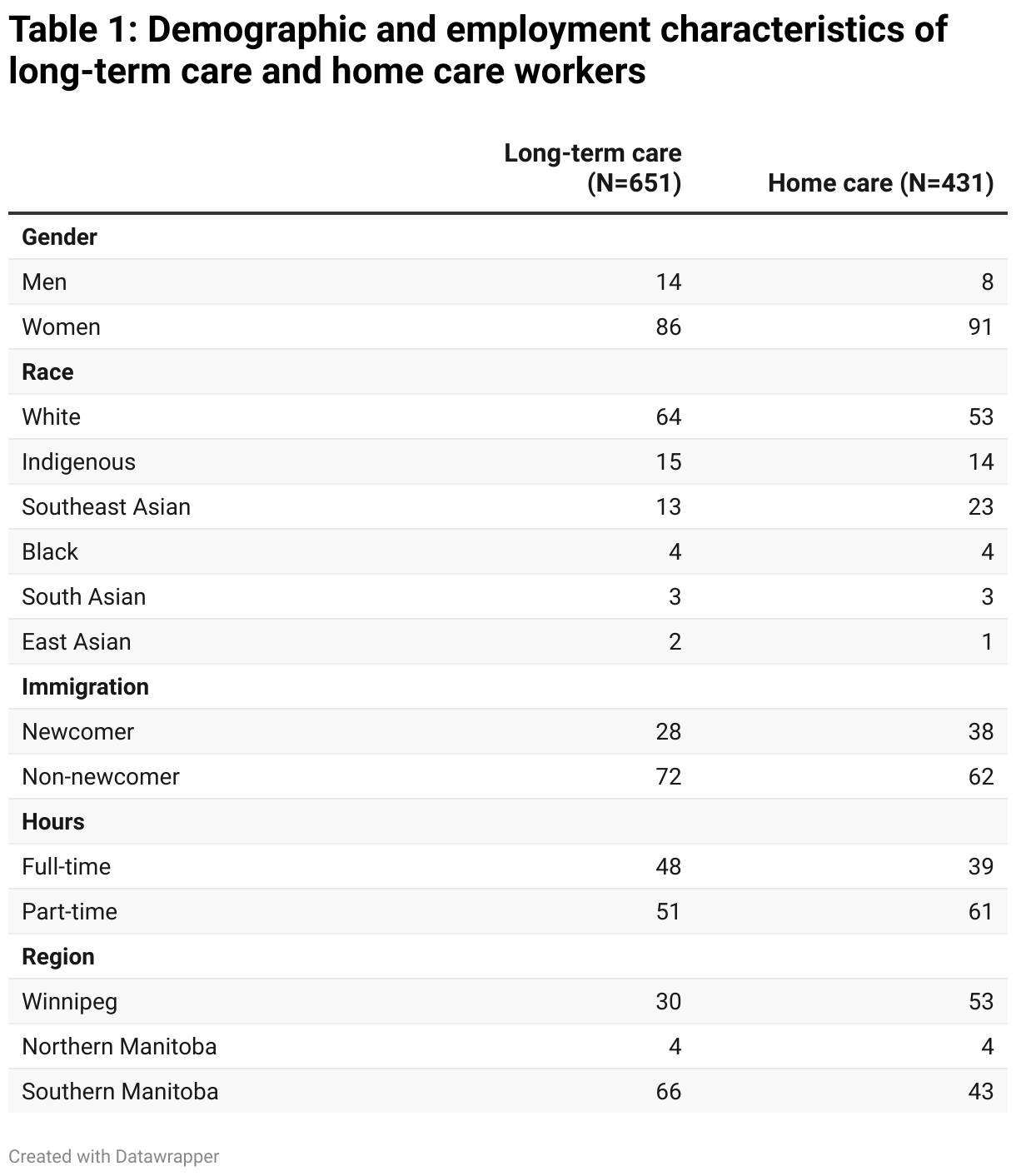
As is typical across Canadian care work settings, the surveyed staff in Manitoba’s long-term care and home care systems were overwhelmingly women (86 percent in long-term care, 91 percent in home care). While the gender composition of long-term care and home care heavily skews towards women, the racial composition of respondents was highly diverse. Over one-third of long-term care staff identified as non-white (36 percent) along with over half of home care workers (47 percent). Amongst racialized continuing care workers the largest groups were Southeast Asian and Indigenous staff, with large shares of Indigenous staff working in Northern Manitoba. Further, many workers self-identified as newcomers to Canada (28 percent in long-term care, 38 percent in home care).
These survey results likely underrepresent the share of racialized and im/migrant workers in Manitoba’s continuing care sector. Previous studies have found that around 70 percent of staff in Manitoba PCHs and 60 percent of staff in home care were born outside of Canada (Toews 2016; El-Bialy et al. 2022). The underrepresentation of im/migrant and racialized workers should be noted as a limitation of this survey.
Job quality: wages, benefits, and risks on the job
Staff within long-term care and home care tend to be precariously employed, with the majority of staff working on a part-time or casual basis (49 percent in long-term care, 59 percent in home care).
While part-time or casual hours have been a draw for some workers, particularly women who are caring for children or other family members at home, many workers reported wanting more hours. Newcomers especially wanted more shifts, with 21 percent indicating they wish to work many more hours. This echoes a repeated call from home care workers for more regular, full-time hours in the public system (Nicholson and Hande 2023).
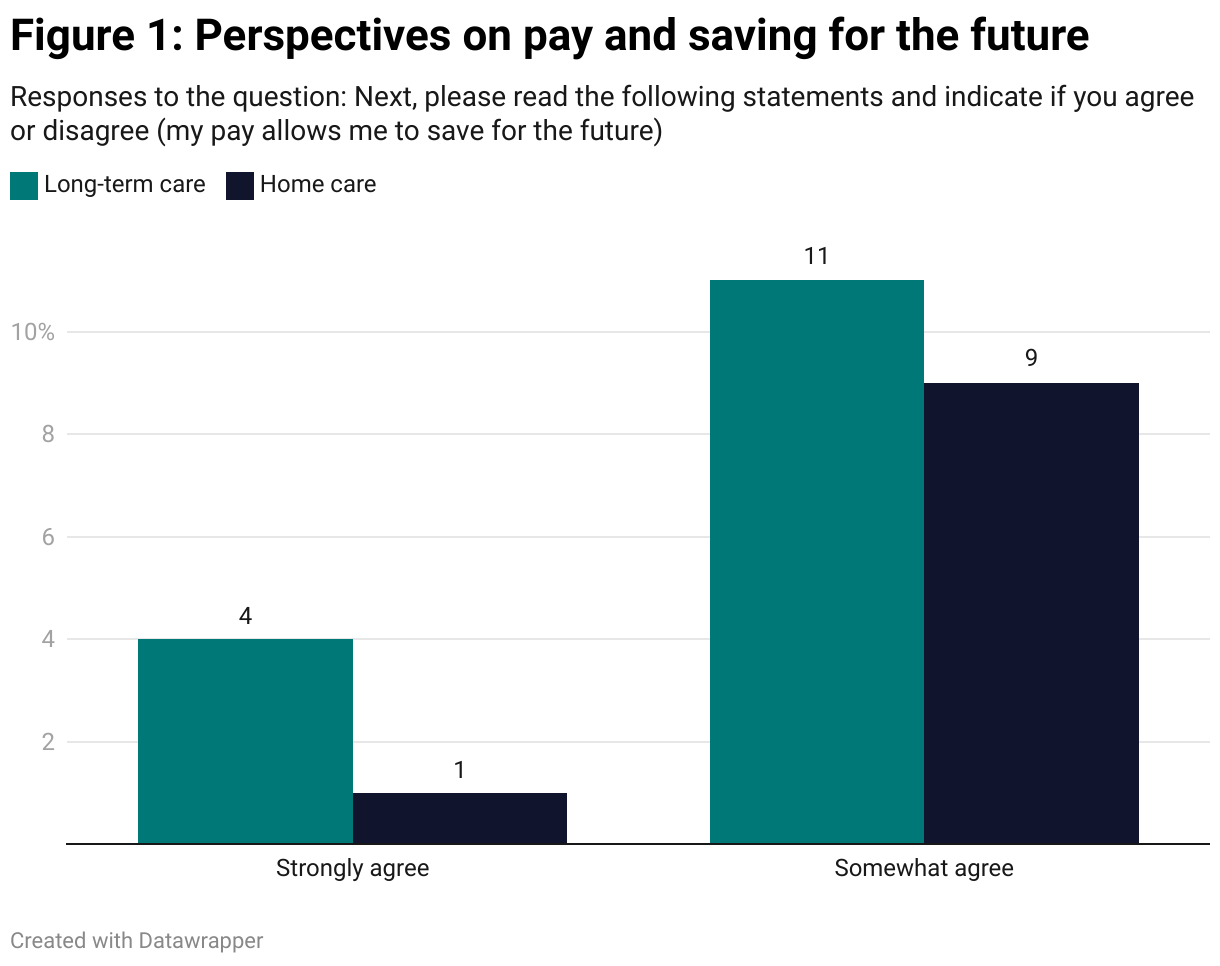
The average hourly wage across long-term care and home care was $20.19, which is $3.81 below Manitoba’s $24 per hour median wage (Statistics Canada 2023). Salaries ranged from $18.87 to $21.04, and were lowest among younger workers. At $18.87 per hour the starting wage for continuing care worker staff surveyed was just above the living wage for Winnipeg, which was calculated to be $18.34 in 2022 (Apata et al. 2022). The living wage calculation reflects the minimum income required to afford the necessities of life.
Given these low wages, it is unsurprising that a very small portion of staff feel their job allows them to save money for the future (15 percent LTC staff; 10 percent of HC staff). All continuing care workers in Manitoba received retroactive pay increases following the settlement of their contract negotiations in August 2022, which delivered a 9.75 percent increase over a seven year contract. However, with Manitoba’s annual inflation rate peaking at 9.4 percent in June 2022, the financial space for care workers to save for the future will likely be unchanged (Manitoba Bureau of Statistics 2022).
Both long term care and home care workers were generally unsatisfied with the time off and benefits they receive through their jobs. Less than 14 percent of home care workers felt satisfied with paid sick-time they received. Long-term care workers were far more likely to be satisfied with their paid sick time, however still fewer than half rated these benefits as ‘excellent’ or ‘good’.
Across all benefits (paid sick time, pension plan, extended benefits, vacation time, family leave) fewer than a quarter of home care staff and 51 percent of long-term care workers were satisfied.
A considerable difference in the benefit plans offered to home care workers versus long-term care workers is reflected in the differing levels of satisfaction these two groups of staff reported in their benefits. Unionized long-term care workers in public PCHs are covered under the Manitoba Healthcare Employee Benefits Plan (HEB), which offers extended care coverage, life insurance, disability, and a defined benefits pension plan. Home care workers are covered under a weaker benefits plan called Manitoba Home Care Employee Benefits which only offers life insurance, dental, vision, weekly sick coverage, and a defined contribution pension plan.
A lack of time off and other benefits is possibly contributing to reports of negative physical and mental effects of the pandemic. When asked what impact the pandemic has had on their mental and physical health at work, 75 percent of long-term care staff and 77 percent of home care staff reported a negative effect on their mental health. Further, 67 percent of staff in long-term care and 65 percent in home care reported negative impacts on their physical health at work resulting from the pandemic.
While a majority of long-term care and home care staff feel at least ‘somewhat safe’ from violence, injury, or verbal abuse on the job, there are still mental and physical risks faced by care workers in these sectors, in particular the risk of contracting COVID-19 on the job. Between 54 percent and 74 percent of care workers reported feeling either ‘very safe’ or ‘somewhat safe’ from violence, injury, or verbal abuse on the job, however, less than a quarter reported feeling ‘very safe’ from any of these risks, with only 15 percent of home care workers feeling ‘very safe’ from verbal abuse at work.
Further, six in ten care workers have been injured on the job (61 percent in long-term care, 55 percent in home care), with over a third of workers in both sectors reporting multiple injuries sustained at work (37 percent in long-term care, 33 percent in home care). Four in ten workers have taken more than a week off of work due to a mental or physical health issue caused by their work. These results suggest some dissonance between a self-reported sense of safety relative to instances of injuries at work.
On top of risks of violence, injury, or abuse at work, care workers face a heightened risk of contracting COVID-19 at work. Of the long-term care staff surveyed, 92 percent experienced a COVID-19 outbreak at work, with 44 percent experiencing more than two. Three in ten long-term care workers believe they contracted COVID-19 at work, compared to 21 percent of home care workers.
Understaffed and overworked
Among the clearest trends from the survey was the severe impact of understaffing on working conditions, stress levels, and capacity to provide quality care. Persistent job vacancies and low staffing were a well documented issue in both long-term care and home care prior to the pandemic (Hande and Nourpanah 2019). The stresses of care work during a public health crisis have exacerbated staffing shortages which have remained since the height of the pandemic.
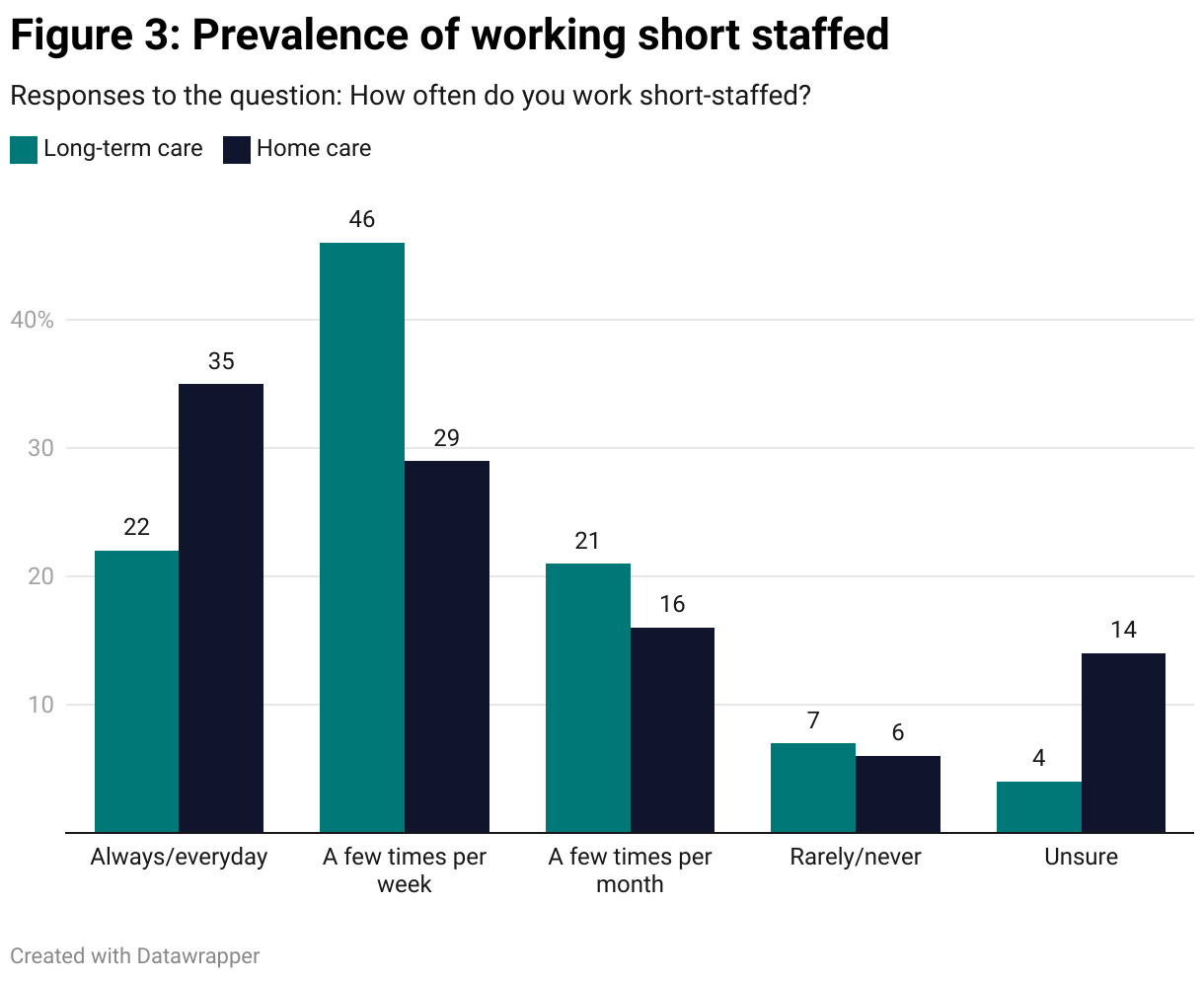
Of staff surveyed, 69 percent in long-term care and 75 percent in home care indicated that staffing levels are worse than they were prior to the pandemic, with around half in both sectors indicating staffing levels are a lot worse. Over two thirds of staff in both sectors (68 percent in long-term care, 64 percent in home care) reported working short staffed at least a few times per week, with 22 percent in long-term care and 35 percent in home care working short on a daily basis. The prevalence of working short indicates a critical staffing shortage across the care sector, contributing to stress and burnout for staff.
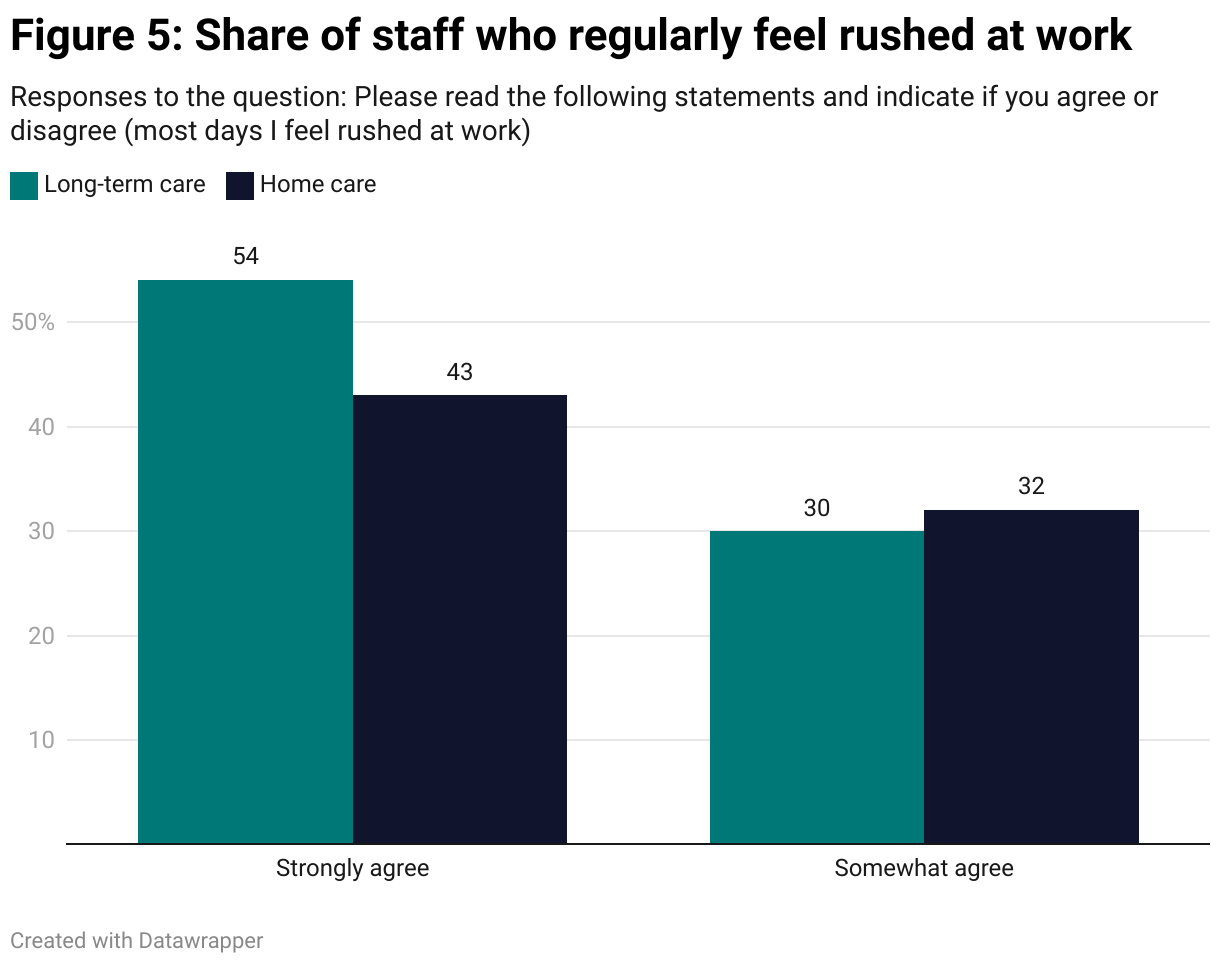
While around two-thirds of respondents agree that they are still able to provide their clients with the care they need, 75 percent of staff in long-term care and 68 percent in home care said that the pandemic has negatively impacted their daily workload. Further, 84 percent of long-term care staff and 75 percent in home care indicated that most days, they feel rushed at work, pointing to an unsustainable workload.
Although a majority of long-term care and home care staff still feel they can provide the care their clients require, the prevalence of feeling rushed at work and working short-staffed indicates that capacity is being stretched unsustainably. It is important to emphasize the damaging psychological effects persistently working short can have on healthcare workers.
Staff in Manitoba PCHs have reported that an inability to provide adequate care or attention to clients can lead to pervasive feelings of guilt or sadness in staff (CUPE 2015). Compounded over time, these feelings can lead to exhaustion and burnout, or what is often termed ‘moral injuries’. Moral injuries emerge from experiences that conflict with a moral sense of right and wrong (Phoenix Australia 2020).
Instances of moral injuries amongst healthcare workers have been increasing since the onset of COVID-19. An all too common example of an instance that could lead to a moral injury is being unable to provide care to someone in need, leading to anger or guilt. At the same time, rushing clients through tasks, meals, or other care activities also lead to increased client agitation and client-to-worker violence.
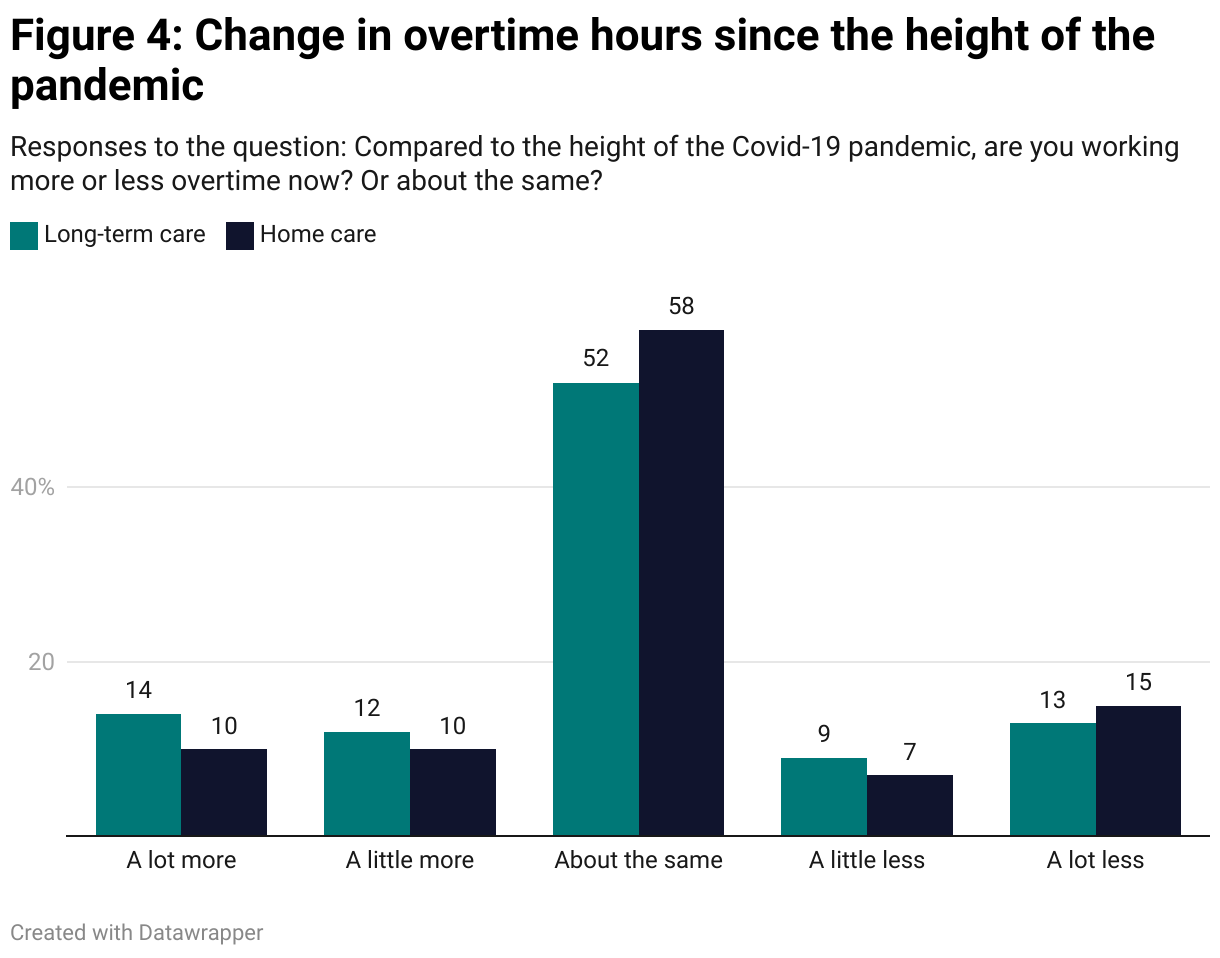
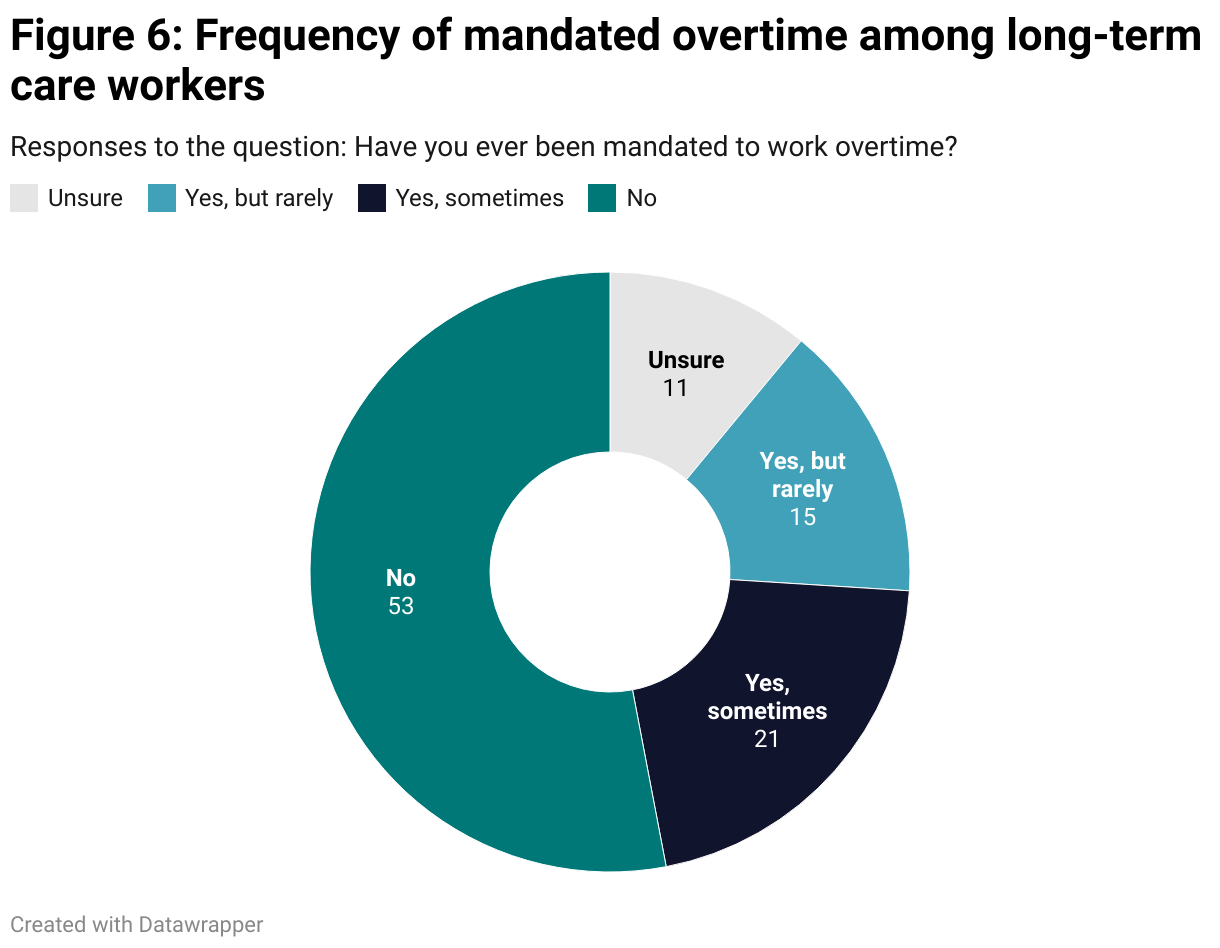
A view of overtime hours adds further evidence that current staff are being overextended to keep care facilities and programs operational. In both long-term care and home care, 78 percent of staff reported working about the same or more overtime than during the height of the pandemic, with 26 percent of long-term care staff and 20 percent for home care staff reported working more overtime in July 2022 than they did at the height of the pandemic. At the same time, 46 percent of long-term care staff reported working mandated overtime, with 10 percent being mandated to work overtime often.
Mandated overtime, along with higher average weekly overtime hours worked, was much more common among young workers and those from Southern Manitoba. The average number of weekly overtime hours for Southern Manitoba long-term care workers was 6.2 hours, nearly double the average amongst Winnipeg staff (3.2 hours). This indicates a more acute staffing shortage in Southern Manitoba.
Privatization and the future of care work in Manitoba
Long term care and home care appear to be undergoing a tried and tested method of stealth privatization that has been applied to healthcare in Canada for the last 30 years. The hallmark of this method is the chronic underfunding of public healthcare services and using the gaps created in the system to justify handing over public services to the private sector (Armstrong and Baines 2020). This method of privatization is what care work scholars Pat Armstrong and Marjorie Griffen Cohen call the ‘private healthcare zombie’: an idea that has long been killed by evidence, but keeps re-emerging from the grave (Cohen and Armstrong 2023).
Of workers surveyed, 70 percent of long-term care workers reported that private agency staff are used in their workplaces every day or a few times per week. Reports of private agency staffing were highest amongst staff who work short on a daily basis. In home care, the number of staff reporting private agency usage was much lower at 23 percent, however the independent nature of home care work makes it harder to get a sense of who one’s coworkers are—this was reflected in 35 percent of staff saying they are unsure about the use of private agency staff.
Decades of research is clear that handing over public healthcare services to the private sector is more expensive and can reduce the quality of care (Armstrong et al. 2019). Quebec has tripled its spending on private agency staff over the last three years to fill shortages created by workers leaving due to fatigue and burnout (Grillo 2022). In many cases, workers are leaving the public system due to low pay and excessive overtime, only to return through a private agency where pay is higher and staff can better manage their own schedules.
Less than a third of workers surveyed in either long term care or home care indicated that they were likely to work for a private agency in the future (27 percent in long term care, 26 percent in home care), though there was a significant regional difference in this response. Forty percent of LTC staff in Winnipeg said they are likely to work for an agency in the future, compared to 24 percent in Southern Manitoba.
Perhaps the most concerning results within the survey were the intentions of care workers to stay or leave the profession in the coming years. Thirty-six percent of long term care staff and 37 percent in home care indicated that they were very likely to leave the profession in the next five years. A further 24 percent in long term care and 26 percent in home care said they were somewhat likely to leave in the next five years. The loss of over half of staff in the coming years would be devastating for long term care and home care services, exacerbating staffing shortages and speeding up staff turnover at a time when population aging will increase demand.
Desires to leave the long term care and home care professions were highest among older workers with 20 years or more of experience and those who work short staffed on a daily basis. This indicates that under current circumstances a wave of retirements and resignations are likely around the corner. A strong correlation between intentions to leave and working short indicate that working conditions and workload are a driver of staff losses.
What would it take to once again build a nation-leading continuing care system in Manitoba?
Since the Stevenson Review’s release, the provincial government has made a number of investments in the home care and long-term care sectors, however these announcements have not gone far enough to meet the staffing levels long advocated for by healthcare workers.
In April 2022, the government announced $15 million would be made available to hire infection control staff and quality control and standards officers to monitor PCHs (Allen 2022). This announcement was followed up in June 2022 by a $16 million investment to allow RHAs to hire 350 HCAs and 72 nurses to bring paid hours of care per day (HCPD) to 3.7 from the previous provincial standard of 3.6 HCPD (Froese 2022a). Advocates have noted that without a more comprehensive recruitment and retention plan, RHAs will struggle to hire hundreds of qualified HCAs, underlining the need for a far more comprehensive strategy.
These investments are welcome, however they remain destined to leave clients and residents lacking adequate direct care while continuing care workers will continue to struggle with inadequate staffing levels. To build a continuing care system capable of meeting the needs of an aging population, much larger investments in staffing and working conditions are required. An ongoing annual investment of $180.8 million into Manitoba’s public continuing care system would be capable of once again building long-term care and home care programs that act as leaders to other Canadian provinces.
Using the Manitoba government’s estimate that a $16 million increase in provincial expenditure is required to increase paid daily hours of care in PCHs by 0.1 hours, an investment of $128 million in PCH staffing expenditure would provide adequate funding to increase paid daily hours of care to 4.5 HCPD. This would bring paid daily hours of care in Manitoba PCHs within the daily direct care hours range of 4.3 to 6.8 hours recommended by researchers, and in line with the latest recommendations from CUPE for 4.5 HCPD (CUPE 2015; Harrington et al. 2020). Within home care, an investment in staffing expenditure of $52.8 million per year would allow RHAs to hire an additional 800 home care aides (HCAs) and home support workers (HSWs), bringing staffing in line with recommendations made in the 2016 Future of Homecare Services report (Toews 2016). Additional investments in training and working conditions should be made to attract staff to the sector.
While an investment of $180.8 million would be the largest investment in continuing care in decades, this level of funding is certainly possible within the Province of Manitoba’s current fiscal outlook. Provincial revenues increased by $2.2 billion in the 2023/24 budget year, including a $1.04 billion increase in federal transfers payments. With a shift in government priorities away from tax cuts, such as the $453 million that will be spent on the education property tax rebate in 2023/24, the Government of Manitoba could increase funding for continuing care without adding to the provincial deficit.
Policy recommendations
The following are the recommendations based on the Probe Research survey results and CCPA analysis to bring Manitoba’s public continuing care services up to evidence-based standards of care:
Raise daily hours of care to 4.5 HCPD—$128 million
In March 2021, Ontario committed $1.9 billion to bring daily hours of care at its long-term care homes up to 4 hours per day by 2025, putting pressure on Manitoba to raise its standard from 3.6 HCPD. Since 2021, Manitoba has only committed to raise hours of care to 3.7 HCPD, well below what long-term care advocates deem acceptable. The research is clear that at least 4.1 HCPD dramatically improves patient care while protecting staff from the harmful working conditions that come from working short, which ultimately lead to burnout (CUPE 2015). To act on the findings of this research, the Minister of Seniors and Active Living should work with RHAs to increase HCPD to 4.5. Building upon the provincial governments 2022 investment of $16 million to raise HCPD from 3.6 to 3.7, raising HCPD to 4.5 should cost $128 million, about 1.6 percent of the total provincial health budget.
Hire 800 more HCAs/HSWs across the home care system—$52.8 million
To reduce wait times for new home care clients, and to ensure clients are receiving the full care they require, more staff must be added to the home care system. The 2016 Future of Home Care Services report was clear that 90-100 new HCAs/HSWs must be hired annually to meet growing demand and higher acuity clients as a result of population aging. Access to information requests indicate that home care funding and hours of care have in fact declined since 2016 (Da Silva 2022). Working back to 2016, hiring 800 HCAs/HSWs would bring us in line with recommendations from the Future of Home Care Services report. Based on an average salary cost for HCAs/HSWs of $55,000, plus 20 percent for benefits ($60,000), $52.8 million is needed to hire 800 more HCAs and HSW across the home care system.
Improve working conditions and benefits for continuing care workers
The Province should improve benefits for long-term care and home care workers to enhance recruitment and encourage workers to choose continuing care as a career. Home care workers should be brought into the Manitoba Health Employee Benefits program to improve extended care and pension benefits. Full-time workers in continuing care secured at least 10 days of paid sick leave in their latest collective agreement, however these benefits should be extended to part time staff. At the same time, all workers in continuing care require improved vacation days, and job security. Full-time, regular hours should be made available for all continuing care workers who wish and efforts should be made to ensure all workers earn above a living wage.
Staff working in privately owned PCHs do not receive access to the same benefits and pension plans that workers in publicly owned facilities access, despite doing work in the public system. Private, for-profit PCH operators should be required to extend the same benefits and pension plans to their own staff that other PCH workers receive.
Further recommendations
Provide tuition support and a living stipend for individuals training to become HCAs/HSWs
RHAs and PCHs have already noted a shortage of skilled HCAs and HSWs in the province. Hiring additional staff will require a large-scale workforce training program. Presently, HSW and HCA positions require one year of training, often through private colleges charging high tuition rates. Many people interested in moving to these positions do not have the savings or work flexibility required to retrain without financial support. The Province launched a tuition support program in July 2022 for uncertified HCAs already working in long-term care who wish to become certified (Government of Manitoba 2022b). This program should be expanded to provide tuition funding for all individuals who wish to train as HCAs or HSWs, regardless of immigration status, as well as living expense support to attract workers without savings or security to take time off for training.
To lower costs, these training programs should be brought into the public system. Training programs for HCAs and HSWs could be offered through existing public adult education institutions, public colleges, or even through regional health authorities themselves where access to on the job training could be streamlined.
Create a fleet of vehicles for home care workers
Home care workers travel to clients homes to provide service, driving many kilometers in a shift. Low mileage reimbursement was a consistent concern in our survey. Mileage payments for home care workers barely cover the costs of gas for a personal vehicle, let alone the costs of maintaining for leasing a vehicle, meaning home care workers are required to own and operate their own vehicle for work. This further limits the pool of workers who can take up this work and can force staff to leave if their vehicles require expensive repairs. Funding should be made available for RHAs to provide home care workers with vehicles for use on the job. Given the high and rising cost of gasoline, these provincial vehicles should be hybrid or electric to meet GHG emission reduction goals.
Create a Seniors Advocate to review long-term care and home care programs
Following recommendations of the Manitoba Health Coalition, the Province should launch an independent seniors advocate to investigate systemic issues in seniors care and make policy recommendations (Manitoba Health Coalition 2023).
Legislate daily hours of care
Manitoba’s Department of Seniors and Long-Term Care has set a provincial target of 3.8 HCPD in Manitoba PCHs. Some advocates argue that actual paid direct care hours are far below this level (Halmarson 2023). Manitoba should follow the lead of other provinces in legislating paid daily hours of care.
Phase out for-profit PCHs
The experience of COVID-19 has made clear the deficiencies in for-profit management of PCHs. The Province of Manitoba should create a strategy to phase out for-profit PCHs while strengthening the public and non-profit continuing care system.
The Government of Saskatechewan effectively phased out private, for-profit long-term care in 2022 through an agreement between the Saskatchewan Health Authority and Extendicare (Ellis 2022). This decision came following deadly outbreaks of COVID-19 in all five Extendicare facilities throughout Saskatchewan during the heights of the pandemic.
Improve the path to permanent residency for im/migrant workers in continuing care
Manitoba’s continuing care system is staffed by a high proportion of im/migrant workers with precarious status. Following the recommendations of Hande and Nourpanah (2019), the province should expedite the path to permanent residency for immigrant workers as part of recruitment and retention efforts. This should be achieved through collaboration between the departments of health, seniors and long-term care, and immigration.
Create a Workers Action Centre to address racism in continuing care
Following the recommendations of Nicholson and Hande (2023), the Province should fund an independent Workers Action Centre to advocate for workers experiencing racism at work, and to help migrant workers navigate the immigration system.
Conclusion
Well-supported care workers are critical to providing the high-quality service that Manitobans expect from their healthcare system. Increasing staffing levels should be a priority to reduce workloads, reduce stress, and improve patient care. Improving working conditions, through improved benefits, better wages, improved immigration supports, and regularizing work encourage staff to remain in their positions, improving outcomes for clients. At the same time, improved oversight and advocacy will further improve the quality of care Manitobans receive.
While the use of private agency staff can fill the gap in staffing levels in the short term, this form of contracting out in the long-term is more expensive for the public sector and increases the casualization of the workforce. Increased reliance on private staffing agencies should be seen as an attempt to further extend the use of ‘just-in-time’ staffing methods in Manitoba’s long-term care and home care sectors, which have been shown to reduce the continuity of care and undermine patient care (Hande and Nourpinah 2019).
Manitoba’s provincial treasury has benefitted from a $2.2 billion windfall increase in revenues in the 2023/24 budget year, which could easily cover the costs required to build a leading continuing care system. This included a $1.04 billion increase in federal transfer payments, $668 million of which was an increase in health and social transfer payments (Harney 2023a). Healthcare spending committed in Budget 2023/24 did mark a departure from the harsh austerity budgets of 2016-2022, but few investments were made in continuing care (Government of Manitoba 2023b). At the same time, the Province introduced $949 million in tax cuts, the majority of which will benefit high income earners in Manitoba, leaving precious little for improvements to continuing care (Harney 2023b). This is a policy direction which must be reversed in future budget years.
In the 1970s, Manitoba led the country by launching a home care program which was subsequently emulated by provinces across the country. It is time for Manitoba to lead the country again through investments in high-quality public long-term care and home care programs which attract staff back to healthcare.
Works cited
Allen, Jenn. 2022. “Manitoba pledges $15 million towards recommendations from review of deadly Maples outbreak.” CBC, April 06, 2023. https://www.cbc.ca/news/canada/manitoba/stefanson-long-term-care-budget-announcement-1.6410253.
Annable, Kristin. Vera-Lynn Kubinec. Caroline Barghout. Joanne Levasseur. 2021. “For-profit homes have higher COVID-19 death rates among Winnipeg nursing homes.” CBC, March 17, 2021. https://www.cbc.ca/news/canada/manitoba/for-profit-care-homes-coronavirus-deaths-wfpcbc-cbc-1.5952171.
Apata, Michael. Jesse Hajer. Niall Harney. 2022. “Manitoba Living Wage Update 2022.” August 2022. Winnipeg: Canadian Centre for Policy Alternatives.
Armstrong, Pat, Hugh Armstrong, Jacqueline Choiniere, Lowndes, and James Struthers. 2020. “Re-Imagining Long-Term Residential Care in the Covid-19 Crisis.” Ottawa: Canadian Centre for Policy Alternatives.
Armstrong, Pat, Hugh Armstrong, Martha MacDonald, and Malcolm Doupe. 2019. “Privatization of Long-Term Residential Care in Canada: The Case of Three Provinces.” In The Privatization of Care. Routledge.
Armstrong, Pat, and Donna Baines. 2020. “Privatization, Hybridization and Resistance in Contemporary Care Work.” In Working in the Context of Austerity: Challenges and Struggles, edited by Donna Baines and Ian Cunningham, 97–108. Bristol University Press. https://doi.org/10.46692/9781529208689.005.
Armstrong, Pat, and Kate Laxer. 2006. “Precarious Work, Privatization, and the Health-Care Industry: The Case of Ancillary Workers.” In Precarious Employment: Understanding Labour Market Insecurity in Canada, 115–38. Montreal: McGill-Queen’s University Press.
Arulnamby, A. SK Sinha. 2023. “A National and International Jurisdictional Review of Long-Term Care Home Legislation, Policies, Directives and Standards with HSO’s 2023 National Long-Term Care Services Standard.” Toronto: National Institute on Ageing, Toronto Metropolitan University.
Baines. 2021. “The Crises in Long Term Care Work: Neoliberalism, Austerity, and the Chance to Rebuild Post-Pandemic.” The Social Lens: A Social Work Action Blog (blog). March 4, 2021. https://socialwork.ubc.ca/news/the-crises-in-long-term-care-work-neoliberalism-austerity-and-the-chance-to-rebuild-post-pandemic/.
Bergen, Rachel. 2020. “Rapid response team going to Winnipeg care home as 8 new deaths reported.” CBC, November 7, 2020. https://www.cbc.ca/news/canada/manitoba/paramedics-called-to-maples-care-home-1.5794040.
Boscart, Veronique M., Souraya Sidani, Jeffrey Poss, Meaghan Davey, Josie d’Avernas, Paul Brown, George Heckman, Jenny Ploeg, and Andrew P. Costa. 2018. “The Associations between Staffing Hours and Quality of Care Indicators in Long-Term Care.” BMC Health Services Research 18 (1): 750. https://doi.org/10.1186/s12913-018-3552-5.
Brown, Jackie. Amit Arya. Andrew Longhurst. “How can we start to make Canada’s long-term care homes about care, not profit?” Montreal: Institut de recherche en politiques publiques. September 15, 2021. https://policyoptions.irpp.org/fr/magazines/septembe-2021/how-can-we-start-to-make-canadas-long-term-care-homes-about-care-not-profit/.
CBC News. 2015. “Winnipeggers Wait Average of 5 Weeks for Home Care: Auditor Report,” August 5, 2015. https://www.cbc.ca/news/canada/manitoba/auditor-report-finds-major-issues-with-manitoba-s-home-care-program-1.3180343.
—————. 2020. “Ford Faces Blowback after Military Report Reveals ‘horrific’ Conditions at Ontario Long-Term Care Homes,” May 26, 2020. https://www.cbc.ca/news/canada/toronto/covid-19-coronavirus-ontario-update-may-26-1.5584665.
—————. 2023. “Over half of Manitoba health-care workers have considered quitting: report.” April 24, 2023. https://www.cbc.ca/news/canada/manitoba/health-care-workers-burnout-report-manitoba-1.6821278.
Cohen, Marjorie Griffen, and Pat Armstrong. 2023. “It’s Time to Bury the Private Health Care Zombie.” The Tyee, January 5, 2023. https://thetyee.ca/Analysis/2023/01/05/Bury-Private-Health-Care-Zombie/.
Collier, E. C Harrington. 2008. “Staffing characteristics, turnover rates, and quality of resident care in nursing facilities.” Res Gerontol Nurs. 1(3):157-70.
CUPE. 2015. For the care we all deserve: The impact of working short on Manitoba personal care home workers.” Winnipeg: Canadian Union of Public Employees. February 2015.
Da Silva, Danielle. 2022. “Regional Home-Care Spending Falls as Demand Outstrips Funds.” Winnipeg Free Press, October 7, 2022. https://www.winnipegfreepress.com/breakingnews/2022/10/07/regional-home-care-spending-falls-as-demand-outstrips-funds.
Doctors Manitoba. 2022. “New Report Reveals Extent of Physician Shortage in Manitoba.” October 26, 2022. https://doctorsmanitoba.ca/news/physicians-in-manitoba-2022
El-Bialy, Rowan, Laura Funk, Genevieve Thompson, Malcolm Smith, Philip St John, Kerstin Roger, Jamie Penner, and Hai Luo. 2022. “Imperfect Solutions to the Neoliberal Problem of Public Aging: A Critical Discourse Analysis of Public Narratives of Long-Term Residential Care.” Canadian Journal on Aging / La Revue Canadienne Du Vieillissement 41 (1): 121–34. https://doi.org/10.1017/S0714980821000325.
Ellis, Brendan. 2022. “SHA officially in full control of Sask. Extendicare LTC homes.” CTV News Regina, October 12, 2022.
Ferguson, Rob. 2021. “Ontario’s for-Profit Nursing Homes Have 78% More COVID-19 Deaths than Non-Profits, Report Finds.” Toronto Star, January 20, 2021.
Froese, Ian. 2022a. “Manitoba looks to hire 400 more staff at personal care homes.” CBC, June 17, 2022. https://www.cbc.ca/news/canada/manitoba/care-home-manitoba-cp-1.6493047.
Froese, Ian. 2022b. “Pay Bumps Expected for 18,000 Health-Care Support Workers after Manitoba Union Reaches Tentative New Deal.” CBC News, August 30, 2022. https://www.cbc.ca/news/canada/manitoba/pay-bump-health-care-support-workers-manitoba-1.6567196.
Government of Manitoba. 2021. “Media Bulletin: Caregiver Wage Support Program Opens Second Intake Today.” January 11, 2021.
Government of Manitoba. 2022a. “Final Report of the Provincial Implementation Plan for the Stevenson Review.” February 2022. https://gov.mb.ca/asset_library/en/proactive/20222023/maples-care-home-final-report-feb-2022.pdf.
Government of Manitoba. 2022b. “News Release: Manitoba government offers tuition support to uncertified health-care aides to enhance skills.” July 19, 2022.
Government of Manitoba. 2023a. “2021/22 and 2022/23 Rate Tables.” Accessed May 26, 2023. https://www.gov.mb.ca/health/pcs/table.html.
Government of Manitoba. 2023b. “Summary Budget and Financial Updates.” March 2023. https://www.gov.mb.ca/budget2023/summary-budget-and-financial-updates.html.
Grillo, Matt 2022. “Quebec Spending on Private Health-Care Workers up by 335% in Last 5 Years amid Labour Shortage.” CTV News Montreal. Montreal: CTV. https://montreal.ctvnews.ca/quebec-spending-on-private-health-care-workers-up-by-335-in-last-5-years-amid-labour-shortage-1.6020491.
Halmerson, Daniel. 2023. “New proposed long-term care standards call for better staffing, more direct care.” CTV News Winnipeg, January 31, 2023. https://winnipeg.ctvnews.ca/new-proposed-long-term-care-standards-call-for-better-staffing-more-direct-care-1.6254280.
Hande, Mary Jean, and Shiva Nourpanah. 2022. “Putting Continuity in Continuing Care.” Nova Scotia: Canadian Centre for Policy Alternatives.
Harney, Niall. 2023a. “Budget 2023 hands down large tax cuts on the back of increased federal transfers.” PolicyFix. Winnipeg: Canadian Centre for Policy Alternatives. March 2023. https://policyfix.ca/2023/03/07/budget-2023-24-hands-down-large-tax-cuts-on-the-back-of-increased-federal-transfers/.
Harney, Niall. 2023b. “Make no mistake, Manitoba’s Budget tax cuts are a gift to the rich.” Winnipeg: Canadian Centre for Policy Alternatives. March 23, 2023. https://policyalternatives.ca/publications/commentary/make-no-mistake-manitoba-budget-tax-cuts-are-gift-rich.
Harrington, Charlene, Mary Ellen Dellefield, Elizabeth Halifax, Mary Louise Fleming, and Debra Bakerjian. 2020. “Appropriate Nurse Staffing Levels for U.S. Nursing Homes.” Health Services Insights 13 (June): 1178632920934785. https://doi.org/10.1177/1178632920934785.
Health Care Financing and Administration, 2002. “Report to Congress: Appropriateness of Minimum Nurse Staffing Ratios in Nursing Homes: Phase II Report.” Washington, DC: US Department of Health and Human Services.
Health Standards Organization. 2023. “National Standard of Canada (CAN/HSO 21001:2023): Long-Term Care Services.” Ottawa: Health Standards Organization.
House of Commons Standing Committee on Health. 2023. “Addressing Canada’s Health Workforce Crisis.” Report of the Standing Committee on Health. March, 2023. https://www.ourcommons.ca/Content/Committee/441/HESA/Reports/RP12260300/hesarp10/hesarp10-e.pdf
Jansen, Irene. 2011. “Residential Long-Term Care: Public Solutions to Access and Quality Problems.” HealthcarePapers. 10(4):8-22.
Jones, Esyllt. 1996. “The Privatization of Home Care in Manitoba.” Canadian Review of Social Policy, no. 37: 96–98.
LeTourneau, Michele. 2020. “Home Care Workers in Short Supply.” Brandon Sun, November 19, 2020. https://www.brandonsun.com/local/2020/11/19/home-care-workers-in-short-supply.
Loreto, Nora. 2020. COVID-19 Long-Term Care (LTC) Deaths in Canada. Accessed June 15, 2023.
Manitoba Bureau of Statistics. 2022. Consumer Price Index (CPI), June 2022.
Manitoba Health Coalition. 2023. “Manitoba Needs a Seniors Advocate.” Accessed May 26, 2023. https://www.mbhealthcoalition.ca/seniors_advocate.
Manitoba Nurses Union. 2022. “A system on the brink of catastrophe.” July 5, 2022. https://www.manitobanurses.ca/news-events/article/40/a-system-on-the-brink-of-catastrophe
Marier, Patrik. 2021. The Four Lenses of Population Aging: Planning for the Future in Canada’s Provinces. Toronto: University of Toronto Press. https://utorontopress.com/9781442612631/the-four-lenses-of-population-aging.
May, Katie. 2020. “Nearly half of Manitoba pandemic deaths tied to care homes.” Winnipeg Free Press, November 24, 2020. https://www.winnipegfreepress.com/breakingnews/2020/11/24/nearly-half-of-manitoba-pandemic-deaths-tied-to-care-homes
—————. 2023. “Home Care Workers File Grievance over Perceived Contract Delays.” Winnipeg Free Press, January 9, 2023. https://www.winnipegfreepress.com/breakingnews/2023/01/09/home-care-workers-file-grievance-over-perceived-contract-delays.
National Institute on Ageing, 2023. NIA Long-Term Care COVID-19 Tracker. Toronto: National Institute on Ageing, Toronto Metropolitan University. Accessed June 15, 2023.
Nicholson, Leah. Mary Jean Hande. 2023. “Justice for im/migrant home care workers in Manitoba.” Winnipeg: Canadian Centre for Policy Alternatives.
Nourpanah, Shiva, Ivy Bourgeault, Lois Jackson, Sheri Price, Pauline Gardiner Barber, and Michael P. Leiter. 2018. “Intersecting Policy Contexts of Employment-Related Geographical Mobility of Healthcare Workers: The Case of Nova Scotia, Canada.” Healthcare Policy = Politiques De Sante 14 (2): 12–21. https://doi.org/10.12927/hcpol.2018.25690.
NUPGE. 2019. “Home Care Privatization.” Ottawa: National Union of Public and General Employees.
Phoenix Australia—Centre for Posttraumatic Mental Health and the Canadian Centre of Excellence—PTSD. (2020). “Moral Stress Among Healthcare Workers During COVID-19: A Guide to Moral Injury.” https://www.moralinjuryguide.ca/Documents/Moral-Injury-Guide.pdf
Roman, Karina. 2023. “New Voluntary Standards Released for Long-Term Care Homes Devastated by the Pandemic.” CBC News, January 31, 2023, sec. Politics. https://www.cbc.ca/news/politics/long-term-care-canada-standards-pandemic-1.6730780
Scott, Katherine. 2021. “Women, work, and COVID-19: Priorities for supporting women and the economy.” Ottawa: Canadian Centre for Policy Alternatives.
—————. 2022a. “A Bumpy Ride: Tracking Women’s Economic Recovery Amid the Pandemic.” Beyond Recovery: Toward a Gender-Just Economy. Ottawa: Canadian Centre for Policy Alternatives.
—————. 2022b. “The crisis in the care economy shows no sign of letting up.” The Monitor, November 25, 2022.
Shapiro, Evelyn. 1997. “The Cost of Privatization: A Case Study of Home Care in Manitoba.” Winnipeg: Canadian Centre for Policy Alternatives. https://policyalternatives.ca/sites/default/files/uploads/publications/Manitoba%20Office/1997/12/Home%20Care%20Evelyn%20Shapiro.pdf.
Silver, Jim, Tim Scarth, and Lisa Shaw. 1997. “The Cost of Privatization: Olsten Corporation and the Crisis in American For-Profit Home Care.” Winnipeg: Canadian Centre for Policy Alternatives.
Statistics Canada. 2022. “The Daily: Consumer Price Index, June 2022.” July 20, 2022. https://www150.statcan.gc.ca/n1/daily-quotidien/220720/dq220720a-eng.htm
—————. 2023. Employee Wages by Industry, Annual: Table 14-10-0064-01
Toews, Reg. 2016. “Future of Home Care Services in Manitoba.” https://www.gov.mb.ca/health/homecare/future_homecare.pdf.
Tungohan, Ethel. 2021. “How COVID-19 Exposed Canada’s Treatment of Migrant Workers.” OpenDemocracy (blog). January 30, 2021. https://www.opendemocracy.net/en/pandemic-border/how-covid-19-exposed-canadas-treatment-of-migrant-workers/?fbclid=IwAR3a8ouaAwalPkuwelf1QhrNo3_Hyb2lMGuQd7vTQZlv9M02fRmKj-QipNE.
Twomey, Amy. 2014. “Pursuing Different Paths in Long-Term Care: Manitoba, Ontario and the Politics of Commercialization.” Doctoral Dissertation, Trent University.
WRHA. 2022. “Media Release: Home care cancellations.” January 6, 2022. https://wrha.mb.ca/2022/01/06/home-care-cancellations/
Appendix: Home care and long-term care workers survey questionnaire
A. Worker profile and experience
First, we’d like to know a little bit about your work and how it’s going…
A1. Do you primarily work in home care or long-term care?
—Home care
—Long term care/personal support worker
—Both
—Neither (THANK AND TERMINATE WITH: Thank you so much for your interest, but this survey won’t be very relevant to you if you’re not a home care or long-term care worker.)
A1a. FOR LTC WORKERS ONLY IN A1 Do you work in more than one facility?
—Yes
—No
A2. How many years have you been working in home care/long-term care? OPEN ENDED
—_____ years
—Unsure/prefer not to say
A3. Why did you choose to work in home care/long-term care? OPEN ENDED
—___________________
—Unsure/prefer not to say
A4. How would you describe your working hours? Are you…
—Full time
—Part time
—Casual
—Unsure/prefer not to say
A5. Do you get enough hours? Or would you like to work more hours in home care/long-term care?
—Would like to work a lot more hours
—Would like to work a few more hours
—I work the right number of hours for me
—I would like to work fewer hours
A6. Thinking of the year so far—say, since January 2022—about how many hours of overtime do you work, if any, in a typical week?
—____ hours of overtime
—None
—Unsure/prefer not to say
A7. And, compared to the height of the COVID-19 pandemic, are you working more or less overtime now? Or about the same?
—A lot more overtime now
—A little more overtime now
—About the same
—A little less overtime now
—A lot less overtime now
A8. LTC WORKERS ONLY And, have you ever been mandated to work overtime?
—Yes, often
—Yes, sometimes
—Yes, but rarely
—No
—Unsure/prefer not to say
A9. Are staffing levels better, the same or worse than before the COVID-19 pandemic?
—A lot worse
—A little worse
—About the same
—A little better
—A lot better
A10. How often do you work short staffed?
—Always/every day
—A few times per week
—A few times per month
—Never/rarely
—Unsure/prefer not to say
A11. Please indicate your hourly rate of pay.
—$_____ per hour
—Unsure/prefer not to say
A12. What about pensions and benefits? Please read the following list and indicate whether you feel this workplace benefit is excellent, good, fair or poor.
ROWS—RANDOMIZE
—Paid sick time
—Pension
—Extended health benefits
—Vacation time
—Family leave (time off to care for kids, elderly parents, etc.)
COLUMNS
—Excellent
—Good
—Fair
—Poor
—Unsure
—I don’t have this benefit
A13. Have you ever taken more than a week off work for a mental or physical health issue you feel was caused by your work? This could be stress leave or disability leave or some other type of sick time.
—Yes
—No
—Unsure/prefer not to say
A14. Have you ever been injured on the job?
—Yes, once
—Yes, more than once
—No
—Unsure/prefer not to say
A15. How safe, if at all, do you feel at work…? RANDOMIZE
ROWS
—From violence
—From injury
—From verbal abuse
COLUMNS
—Very safe
—Somewhat safe
—Somewhat unsafe
—Very unsafe
—Unsure/prefer not to say
B. Views and attitudes on quality of care
B1. Next, please read the following statements and indicate if you agree or disagree. RANDOMIZE
ROWS
—I’m able to give my clients the kind of care they need.
—I would encourage my kids—or the kids in my life—to work in home care or long-term care
—My pay allows me to save for the future
—I have the equipment I need to do my job properly
—I get the training I need to do my job properly
—The good things about my job outweigh the bad
—Most days, I feel rushed at work
—I have time to really get to know my clients
COLUMNS
—Strongly agree
—Somewhat agree
—Neither agree nor disagree
—Somewhat disagree
—Strongly disagree
—Unsure/prefer not to say
C. Experience during COVID-19
Next, a few questions about your experience during the COVID-19 pandemic…
C1. What kind of impact, if any, did the last two years of the pandemic have on the following aspects of your job?
ROWS
—Your mental health
—Your physical health
—Your daily workload
COLUMNS
—Very positive impact
—Somewhat positive impact
—Somewhat negative impact
—Very negative impact
—No real impact
—Unsure/not applicable
C2. LTC WORKERS ONLY How often, if at all, were there outbreaks of COVID-19 at your workplace?
—Never
—Once
—Twice
—More than twice
—Unsure/prefer not to say
C3. Which one best describes your experience?
—I tested positive for COVID-19 and believe I contracted the illness while working in health care
—I tested positive for COVID-19 but believe I contracted the illness outside of work
—I believe I had COVID-19 but did not get tested/tested negative
—I have not had COVID-19
—Other (please specify): _________________
C4. LTC WORKERS ONLY During the pandemic, were you redeployed to another workplace or to a different job against your wishes?
—Yes, often
—Yes, sometimes
—I was redeployed but I was comfortable with that
—No
—Unsure/prefer not to say
C4a. LTC WORKERS ONLY And, were you affected by a single-site order during the pandemic that prohibited you from working in more than one facility?
—Yes
—No
—Unsure/prefer not to say
C5. HOMECARE WORKERS ONLY During the pandemic, were you redeployed to a different job or to care for a different set of clients against your wishes?
—Yes, often
—Yes, sometimes
—No
—Unsure/prefer not to say
D. Experience and interest in private agency work
Next a few questions about private agencies…
D1. LTC WORKERS ONLY Thinking about your own workplace, how often, if at all, are private agency staff used?
—Always/every day
—A few times per week
—A few times per month
—Never/rarely
—Unsure/prefer not to say
D2. HOMECARE WORKERS ONLY Thinking about your current experience in home care, how often, if at all, are private agency staff used to deliver home care?
—Always/every day
—A few times per week
—A few times per month
—Never/rarely
—Unsure/prefer not to say
D3. Based on what you know and see, is the care offered by private agency staff generally…
—Excellent
—Good
—Fair
—Poor
—Unsure/prefer not to say
D4. How likely or unlikely are you to work for a private health care agency that provides home care or long-term care workers—either part-time or full-time?
—Very likely
—Somewhat likely
—Somewhat unlikely
—Very unlikely
—Already work for a private health care agency
E. Future plans
E1. What about the future? How likely are you to leave home care or long-term care in the next five years?
—Very likely TO E2
—Somewhat likely TO E2
—Somewhat unlikely SKIP TO DS
—Very unlikely SKIP TO DS
—Unsure/prefer not to say SKIP TO DS
E2. Why are you likely to leave home care/long-term care in the next five years? Please read the list below and choose your top three reasons in order of importance. RANDOMIZE
—Pay
—Lack of contract
—Dangerous patients
—Scheduling/schedule
—Just not for me
—Low milage rate
—Poor benefits (pension, health insurance, etc.)
—Not enough sick time
—Lack of afterhours support
—Lack of respect/equity
—Other: Please specify______________________________
DS. Demographics
Last few questions now—we want to know a little more about you, in part to make sure we’re hearing from all kinds of health care workers.
DS1. How would you describe your gender? Are you…?
—Male
—Female
—Prefer to self-describe (gender-fluid, non-binary, two-spirit): ____________
DS2. Which category best describes your age?
—18-34
—35-54
—55-60
—60+
DS3. What are the first 3 characters of your postal code? This is to ensure Manitobans from all areas of the province are included. (DROP DOWN LIST ONLINE)
—__ __ __
DS4. What is the highest level of formal education you have completed?
—Grade school/some high school
—Completed high school
—Some apprenticeship or trades training
—Journey-person certification
—Some community college
—Completed community college diploma
—Some university
—Completed university undergraduate degree
—Completed graduate/professional degree
—Prefer not to answer
DS5. Do you identify yourself as an Indigenous person? Here we are including status or non-status First Nations, Métis or Inuit?
—Yes
—No
—Unsure/Prefer not to answer
DS6. Were you born in Canada?
—Yes
—No
—Prefer not to answer
DS7. (ASK ONLY OF NON-INDIGENOUS RESPONDENT, THOSE WHO DS1.=NO) Could you please describe your ethnic or cultural origins? This will help us understand how diverse health care workers are in Manitoba.
(For example, Filipino, Canadian, Chinese, Scottish, East Indian, French, Ukrainian, Portuguese, etc.) OPEN ENDED
(PHONE: SOFT CODES—DO NOT READ)
—White
—South Asian (e.g., East Indian, Pakistani, Sri Lankan)
—Chinese
—Black
—Filipino
—Arab
—Latin American
—Southeast Asian (e.g., Vietnamese, Cambodian, Laotian, Thai)
—West Asian (e.g., Iranian, Afghan)
—Korean
—Japanese
—Other group—specify:_______________________
—Unsure/prefer not to answer
DS8. Do you actively care for children or other family members, such as aging parents, on a regular basis?
—Yes, children
—Yes, parents or family members
—Yes, both
—No
—Prefer not to answer
DS9. Prize recontact question
Thank you very much for your time. Those are all the questions we have today.
This publication is part of a larger project, Beyond Recovery, which is working to support and advance a gender-just recovery from the COVID-19 pandemic. The project’s goals are to document and analyze women’s experiences, with a particular focus on those of marginalized women in hard-hit sectors, and to provide evidence-based policy proposals to ensure those who are most impacted in this pandemic are front and centre in Canada’s recovery. Considering differences in the experiences of women with intersecting identities is crucial to understanding the impact of the pandemic and efforts to craft a fair and inclusive recovery, attentive to the experiences and struggles of marginalized and under-represented groups.
This project has been funded in part by Women and Gender Equality Canada.

Notes
- We use the term continuing care to refer to home care, long-term care, and other community-based healthcare focused on aging and outpatient care. Home care and long-term care were brought into Manitoba’s welfare state under the Continuing Care Program (1974) (Shapiro 1997).
Acknowledgements
The author would like to thank the following reviewers for their thoughtful comments on earlier drafts of this paper: Katherine Scott, Molly McCracken, Jess Klassen, Matt McLean, and Andy Regier, as well as two anonymous reviewers. The author would also like to thank the frontline staff who participated in the survey which is central to this paper, both for their generous responses and for their ongoing work in Manitoba’s healthcare system.
Niall Harney (he/him) holds the Errol Black Chair in Labour Issues at the Canadian Centre for Policy Alternatives–Manitoba.