
One of the most persistent population health patterns in history is that those who are better resourced in terms of income, education, social capital or whatever domain, have better outcomes than those who have less. It does not matter what place, historical time period, or context, generally, the best off have always had the best health.
This pattern is the social gradient in health. Population health improves in a stepwise pattern as circumstances improve along the socioeconomic spectrum: Those near the middle tend to do better than those with the least, those with above average resources do better than the middle, those who have the very most generally enjoy better health than those with above average resources.
A popular explanation for this phenomenon is known as the “fundamental causes” theory. Put simply, people with more are healthier because they use their resources to their advantage to achieve and maintain a better health status compared to people who have less.
On the surface, this might not be an obvious problem. Why should society care if some people use their resources to improve their health, or living conditions, or the well-being of their children?
There are two reasons. The first is about fairness. The relationship between health and socioeconomic status endures, regardless of the diseases of the day that are killing us or compromising our health. This raises the question of whether social policy intervention is required on behalf of those who are disadvantaged by the socioeconomic distribution.
The second is efficiency. Living in a more egalitarian society is associated with better health outcomes, and the best off in more equal societies do better than their counterparts in less equal societies. That means that potential health gains are not limited to the recipients of a social intervention.
The fundamental causes
Link and Phelan argue that there are a variety of assets that the best-off use to maintain health: money, of course, but also knowledge, prestige, power, and social networks. Essentially, all the things that come along with being at the top of the social pyramid, which make life easier in small and large ways, are employed to benefit health, resulting in the gradient described above.
Key to the argument is that these advantages are not limited to a single disease, they convey health benefits across multiple behaviours and diseases; having a good diet does not only prevent myocardial infarction, it has global benefits across complicated disease processes that we do not completely understand, nor do we have to understand them to figure out that eating healthy is a good thing and correlates with lower incidence of many diseases.
Most annoyingly, addressing the mechanisms through which these advantages translate into a health outcome does not improve equity in outcomes because new mechanisms arise and become relatively more important in maintaining the health gradient. In other words, were we to somehow equalize diet across society, the gradient would persist because the resource advantage allowing the adoption of health-enhancing benefits still exists; the gradient remains despite action on a specific reason for its persistence. There are simply too many mechanisms, and there always will be. Chasing down every single mechanism becomes an exhausting and impossible mission for public health practitioners.
The realization that these are not end-of-life penalties but life-long health burdens is particularly troublesome. Canadian researchers have long pointed out health outcomes are dominated by social forces and those forces affect us from childhood. Children in high stress environments due to, say, material deprivation, are more likely to become adults with a poorer health profile than other children. Disability and frailty are more common in older adults with lower incomes, and those conditions can take years of exposure to poor environments to manifest.
Finally, there is evidence that resources are the key issue here, so improved material well-being would manifest as better health outcomes. Conditions that we consider to be less preventable (e.g., multiple sclerosis) have a much milder social gradient than those that are preventable (e.g., cancers with known causes or accidental injuries), meaning that when no resources can be mustered to prevent something it is less likely to be concentrated among the poorest. So, while resources cannot explain everything, there is a compelling argument to act upon the fundamental causes of poor health rather than chasing specific mechanisms linked to a disease du jour.
So what?
Some treat the health inequality in society as a sad byproduct of the way we structure society, calling for a reinvention of the way we plan our economy, run our governments, or allocate resources. It is unclear whether radical solutions are called for if the fundamental causes are also driven by non-economic factors, like personal influence. The best a government can do is take action to mitigate the impact of being dealt a bad hand of the social determinants of health by improving the social conditions into which those less fortunate are born, grow, live, work and age.
Governments already do this through spending on their social-serving portfolio. Factors like housing, income level, and the welfare of children are all things that households dedicate resources to if they can afford to. Our work has suggested that the relative return to additional social spending, in terms of population health improvements, could be higher than that same spending on the medical care system. Further, the potential return is higher in jurisdictions with more income inequality.
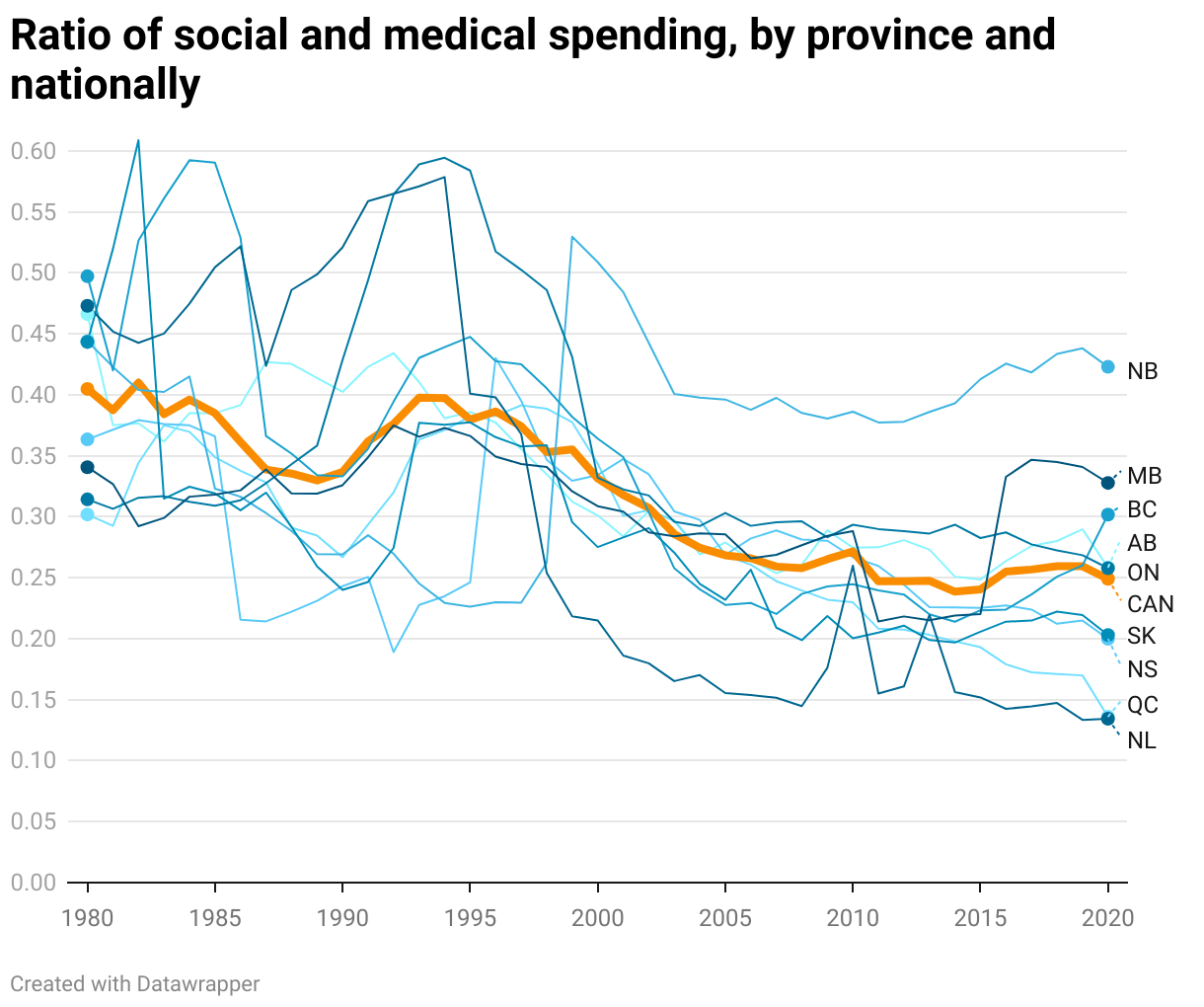
When we monitor spending on social and medical services as a ratio (see the chart below) we can see that in Canada, over time, the overall average (thickest line) is decreasing over time and the individual provinces (thin lines) are moving in the same direction overall—signalling that social spending is declining as a proportion of medical spending. This means that action on the fundamental causes of health among those with fewer resources, especially the poorest, has decreased since the national average’s last highest point in approximately 1993.
To address the factors that essentially limit health equity is to address the existing system of exposure that results in poor health. These systems are multifactorial and the government can act on some of them explicitly through social spending. Due to the constantly changing nature of science, technology, medical care, and government policy priorities, there will always be new mechanisms through which those with more resources can achieve better health outcomes than those who have less.
But it is highly inefficient to rely on the medical system to cover downstream health costs for those left behind when prevention could have been achieved at a lower cost to taxpayers.
Discussion about the correct level of social spending is, at this stage, premature, since social spending has not budged on a per capita basis for decades while medical spending grows on a regular schedule.
Improving population health requires us to reverse this trend by increasing social spending on programs that are already in place and improving the environment that people live in. Social investments need to be prioritized as an investment in health care, because relying on medical care is unnecessarily expensive and saddles so many with unfair health burdens that could have been prevented.

