
There’s more money on the table—but without adequate strings attached, the provinces could end up spending it on tax cuts instead of fixing health care.
Executive Summary
As emergency rooms are overwhelmed, surgery wait times continue to lengthen, and under-resourced childrens’ hospitals face surges related to viral infections like COVID, the provincial and territorial governments have accepted the federal government’s new health care funding deal.
But there’s more than meets the eye with this deal.
It provides an additional $46.2 billion to provinces and territories over the next 10 years, but not all of that money will have conditions attached.
The deal requires provinces to spend 58 cents out of every new dollar on actual new health care programs—barely a majority—while leaving the remaining without requirements.
So what will this new money buy? Not necessarily new health care improvements.
A position paper jointly authored by all of the provinces and territories in 2021 suggests that the provinces’ position coming into the negotiations was a plan to spend zero dollars of the increased federal transfers on higher health care spending. They actually wouldn’t change any operational funding in any department if they got extra federal funding. According to the model they outlined, the provinces and territories would use the extra federal health care money to pay down their deficits—although all of the big provinces now have cumulative surpluses projected for the future.
So despite provincial ad campaigns that show destitute doctors and nurses begging for federal funding, the question of who is responsible for the crisis in Canadian health care is not so clear cut. Health care is a provincial jurisdiction and the big provinces are flush with cash. It’s not money stopping them from fixing their systems, it’s political will.
The federal government can, and should, increase funding to the health care system—but that money shouldn’t have strings attached, it should have chains that ensure new health care money is actually spent on improving health care.
Our content is fiercely open source and we never paywall our website. The support of our community makes this possible.
Make a donation of $35 or more and receive The Monitor magazine for one full year and a donation receipt for the full amount of your gift.
Introduction
With a new 10-year funding deal between the federal government and provincial/territorial governments announced last week, one would think that Canada’s health care woes will soon be remedied.
Think again.
Yes, the federal government has put more money on the table for health care: an additional $46.2 billion in new money will flow from Ottawa to the provinces and territories over the next 10 years. The federal government was already planning an increase of $149.9 billion in federal transfers over the next decade. Including the latest deal, this would result in a total increase of $196.1 billion.
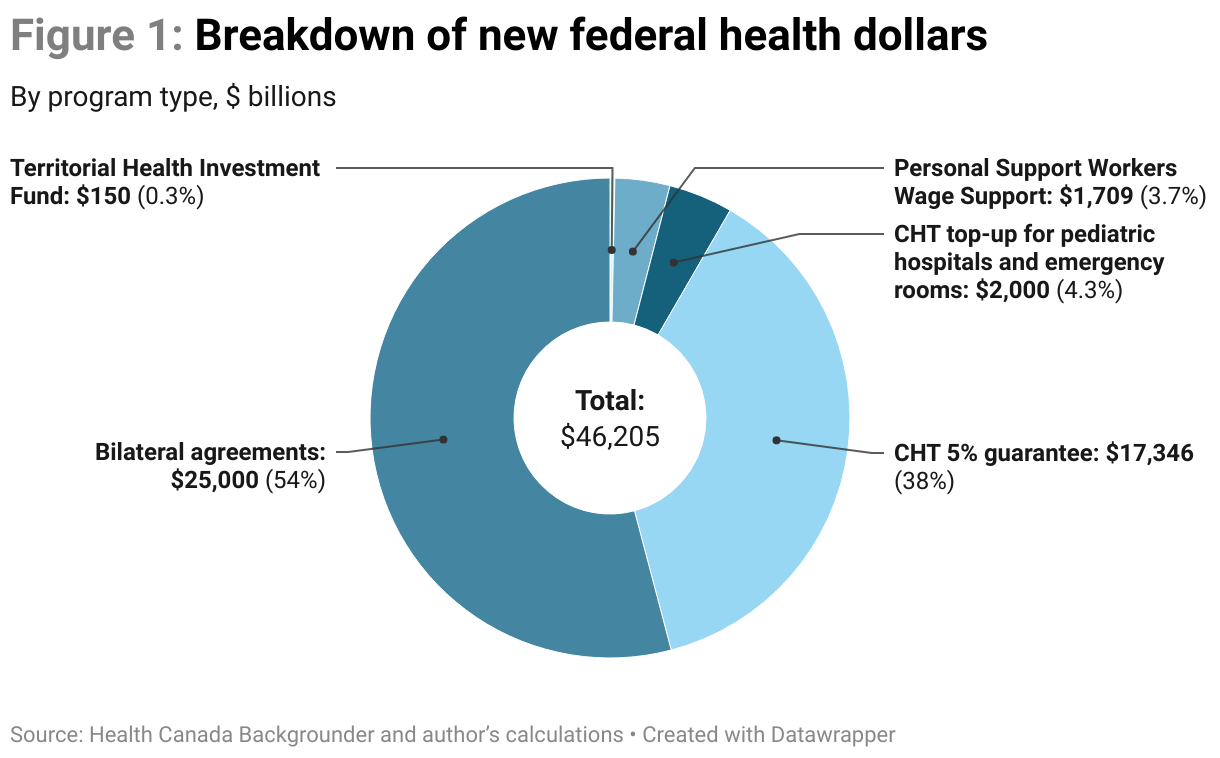
This $196.1 billion package includes new funds across these five areas:
- Guaranteeing Canada Health Transfer (CHT) increases by at least five per cent a year.
- Providing an immediate $2 billion CHT top-up, labelled “pediatric hospitals and emergency rooms.
- A Territorial Health Investment Fund for medical travel costs.
- A personal support worker wage top-up.
- $25 billion for new bilateral agreements with each of the provinces.
How the money will be allocated
The federal government only attached strings to 58 per cent of the new money. That means 58 per cent of that money actually has to be spent on health care—the rest can be spent on whatever the provinces want.
While some federal deals require the provinces and territories to match funding—that is frequently the case with federal infrastructure deals—there is no matching requirement for health care spending in this deal. On infrastructure spending, every dollar of federal funding can easily become two or three dollars of actual infrastructure spending—because the province and municipality are expected to pitch in a third of the funds. With the new health care funding deal, a federal dollar is only guaranteed to become 58 cents in actual health care spending, not two or three dollars. It also means that any new health care programs coming out of this new money will be entirely funded by the federal government.
Bilateral agreements
The health care deal includes $25 billion—over half the package—worth of incremental spending over 10 years to go toward bilateral agreements with the provinces and territories. By “incremental,” the federal government means that provinces and territories have to show that it is actually a new program, not a program that they were going to do anyway and send the bill to Ottawa.
The federal government wants to focus on four areas for upcoming bilateral deals:
- Improved access to primary care.
- Support for health care workers and clearing up surgical and diagnostic backlogs.
- Substance abuse and mental health care.
- Better data and health care systems.
Personal support workers
The pandemic has made crystal clear the importance of personal support workers in the health care system, particularly in long-term care. It has also exposed the terrible working conditions that personal support workers have been expected to tolerate.
This new health care deal focuses on better pay for personal support workers: it includes $1.7 billion worth of additional wage support over five years in a deal that’s similar to the essential workers wage top-up that the provinces rolled out with federal funding in the early stages of the COVID-19 pandemic.
The federal government will require the provinces to spend this new money on higher wages for low-paid personal support workers.
Even where the provinces have to actually spend the money on “new” programs, the federal government has left some wiggle room. Maybe a province was already going to pay personal support workers more and now they can say it’s a “new” program or maybe a province was already going to clear its surgical backlog and it can pitch it as “new” to the federal government. The provinces and territories can certainly play games here, but it’s far better than nothing.
No strings attached: other funding priorities
The personal support workers’ wage top-up and the bilateral agreements account for 58 per cent of the total 10-year funding deal, or $26.7 billion of the $46.2 billion package.
The remaining 42 per cent—$19.5 billion—is not tied to specific spending requirements, which means the provinces and territories will get the money but they won’t have to necessarily spend it on health care. This includes the guaranteed five per cent annual increase in the Canada Health Transfer (CHT) payments, the $2 billion CHT top-up and the territorial travel money.
These programs have suggested uses—like children’s hospitals or territorial health travel—but the federal government is not imposing any requirements for the provinces to use the money as such. It is unconditional revenue for the provinces, without the need for any specific expenditure on the other side.
Essentially, the label on the box of cash says “kids’ hospitals and ERs” but the back of the card says “no receipts required.” Canadians can only hope that the provinces and territories do the right thing, but they might do something entirely different with that money, such as increase their budget surpluses and pay off bondholders in New York, offer massive tax cuts, or whatever.
The Canada Health Transfer has been unconditional since 1995. There is no requirement that the provinces show how they spend the money. They just receive it as an unconditional revenue stream from the federal government.
How much will be spent on health care?
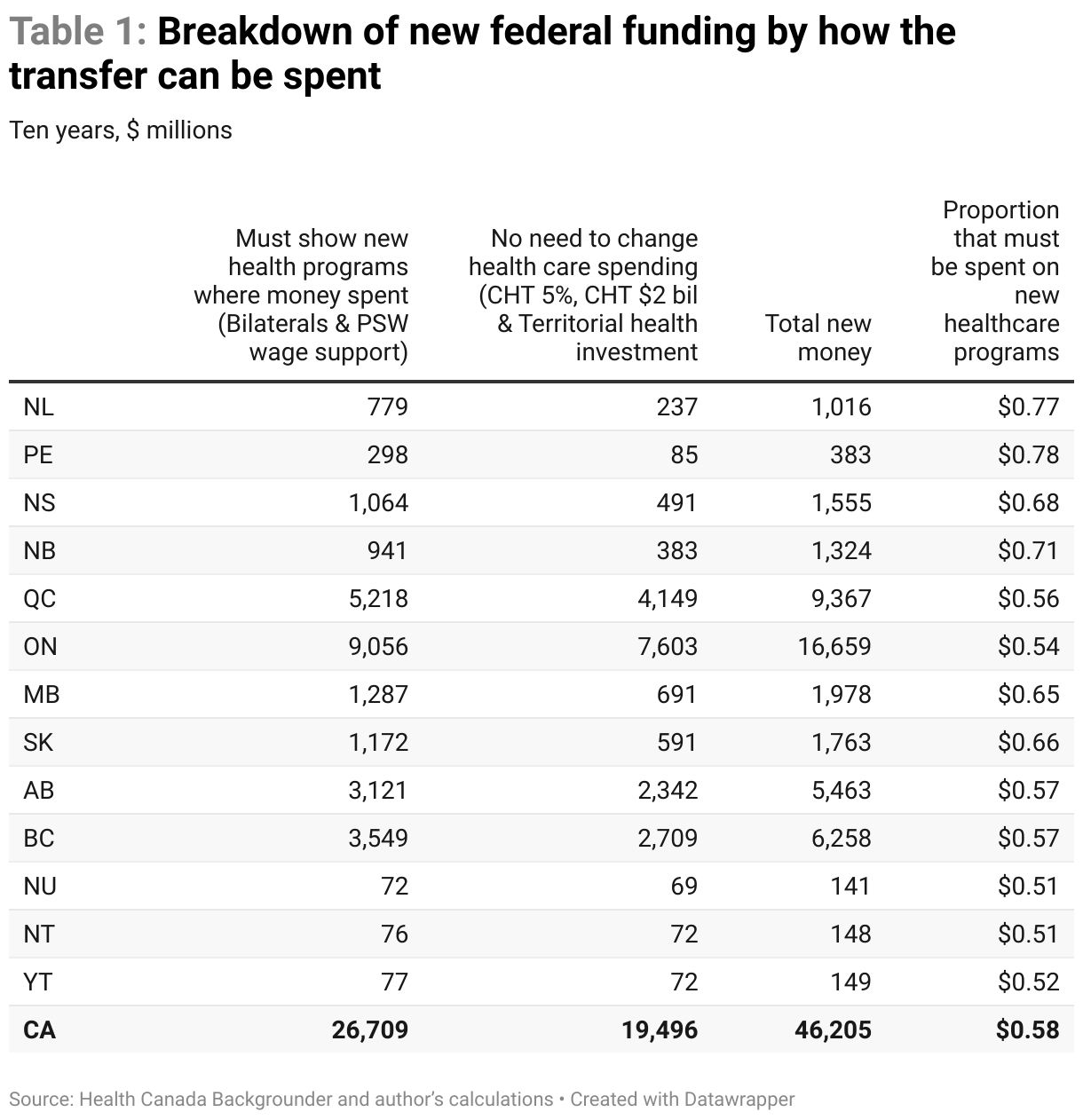
The proportion of new funding that the federal government requires the provinces and territories to spend on health care varies quite a bit by jurisdiction. Across all jurisdictions, 58 cents of every dollar from this new package will have to be spent on new health care programs. Figure 2 lays out that ratio by province.
The federal government is going to require that P.E.I. spend 78 cents out of every new health care dollar from this new package on new health care expenditures that aren’t already in the plans.
The big provinces—notably Quebec and Ontario—will not be required to spend as much of what they receive on health care.1 Of the $16.7 billion in new money that the federal government will send to Ontario over the next 10 years, for instance, the federal government only requires the province to spend $9.1 billion on new health care improvements (or 54 cents of every dollar they receive). The federal government isn’t looking for matching funding; it simply wants 54 cents out of every dollar they send to Ontario to actually be spent on better health care. How much of the rest ends up improving health care will depend on how much public pressure is brought to bear on Queen’s Park.
It’s similar for Alberta and B.C.: the federal government only requires that they spend 57 cents of every dollar on improving health care. Of the $5.5 billion the federal government will send Alberta over the next 10 years, it only requires $3.1 billion to be spent on health care. Of the $6.3 billion the federal government will send B.C., it only requires $3.5 billion to be spent on better health care.
Premiers wanted no strings attached
The federal position is that the provinces only have to spend 58 cents out of every new dollar that they get on health care. But what’s the provincial position?
Two years ago, all of the provinces and territories, except Newfoundland and Labrador, put out a position paper on exactly what they wanted from new health transfers. This was the provincial/territorial starting position: over the next 10 years, they wanted to receive $326 billion, much more than the $46.2 billion that the federal government has on offer.2 That’s obviously a big difference. But there was another, even more revealing element: the proportion of the new health transfers that the provinces/territories would want to actually spend on improving health care.
The provinces wanted to receive an extra $26 billion in the first year, rising to $44 billion in the tenth year. So the revenue difference between the before and after scenarios is exactly those amounts.
What’s truly shocking—and revealing—is the graph of planned provincial/territorial operating expenditures before and after a new federal health transfer.3
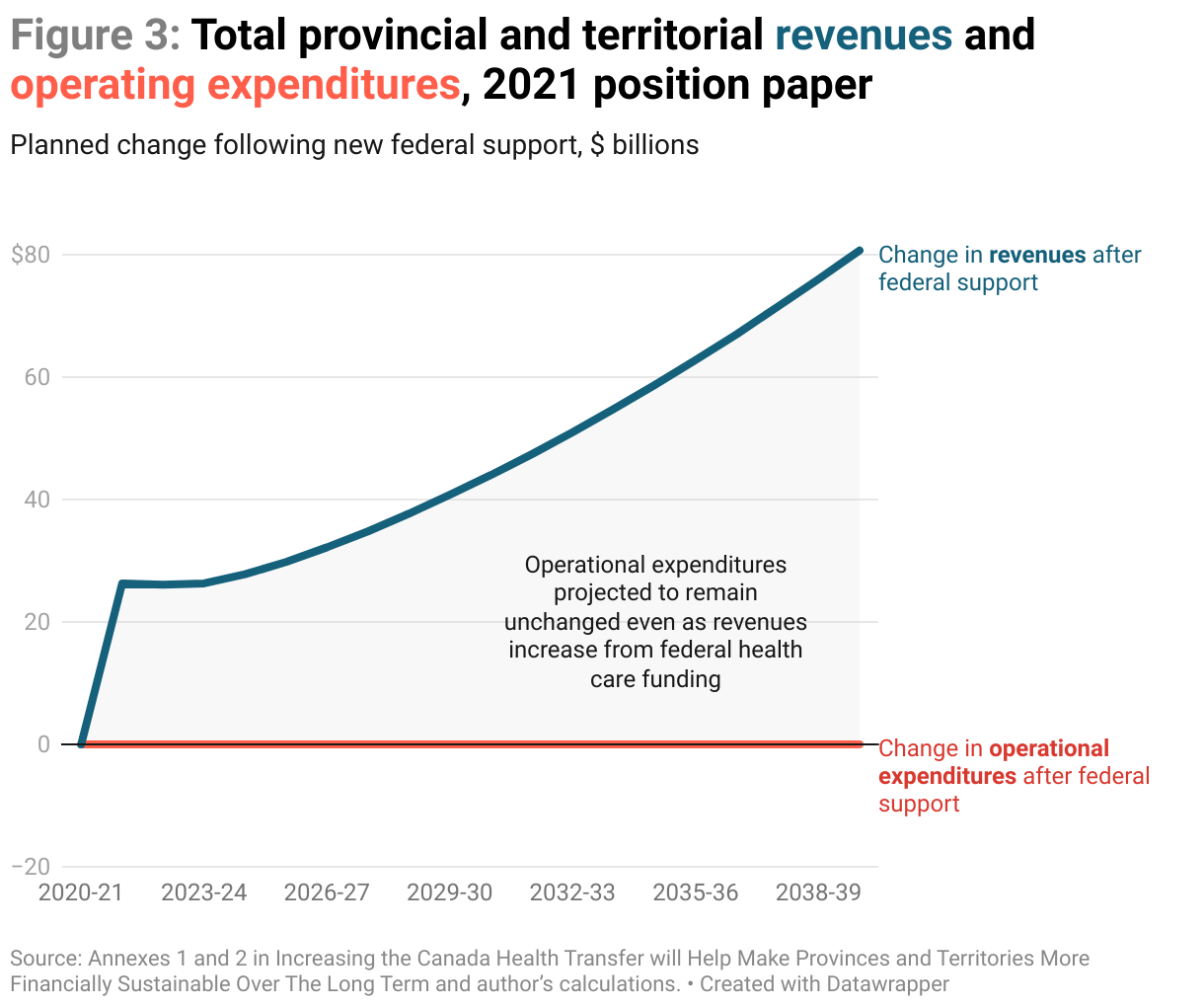
Program expenditures before and after a massive infusion of federal cash are identical! What this means is that whether the provinces and territories receive $26 billion or $44 billion more in federal transfers a year, they haven’t planned to spend an extra dime on health care.
It’s important to note that the provinces and territories are planning to grow their health care budgets, to varying degrees, but provincial leaders have an underlying assumption that their existing health care budgets are adequate to deal with overwhelmed emergency rooms, surgery backlogs, and under-resourced childrens’ hospitals.
The provinces’ and territories’ own position paper shows they had no intention of changing their budgets by even a penny to address these issues.
So while the federal position is that it would like the provinces and territories to spend 58 cents out of every new health care dollar on actual health care, the starting provincial position is that they wouldn’t spend any new federal health care dollars on actual health care. Not one cent.
Not on health care, and not on anything else
But wait, there’s more.
If the provinces’ operating expenditures would remain completely the same even if they receive between $26 billion and $44 billion more a year from the federal government, it’s clear that they didn’t plan any net new spending on anything else either. Not on better education. Not on expanding affordable child care. Not on improving the justice system. Not on post-secondary education.
The position paper explicitly shows that their only intention was to spend additional new federal funding on reducing their own deficits.
Please can I have a bigger surplus
It’s worth noting that the provincial-territorial position paper was written in February 2021, when the provinces were predicting doomsday scenarios for deficits. Those predictions weren’t worth the paper they were written on, they were so off the mark (as I documented in my November 2022 report Flush with Cash).
I’ve updated those figures to February 8, 2023, the day after the federal agreement details were released. Guess what? Nearly every province is projecting a huge surplus for 2022-23—and going forward, as far as the eye can see. What’s the deficit emergency? There is no emergency. Quite the opposite.
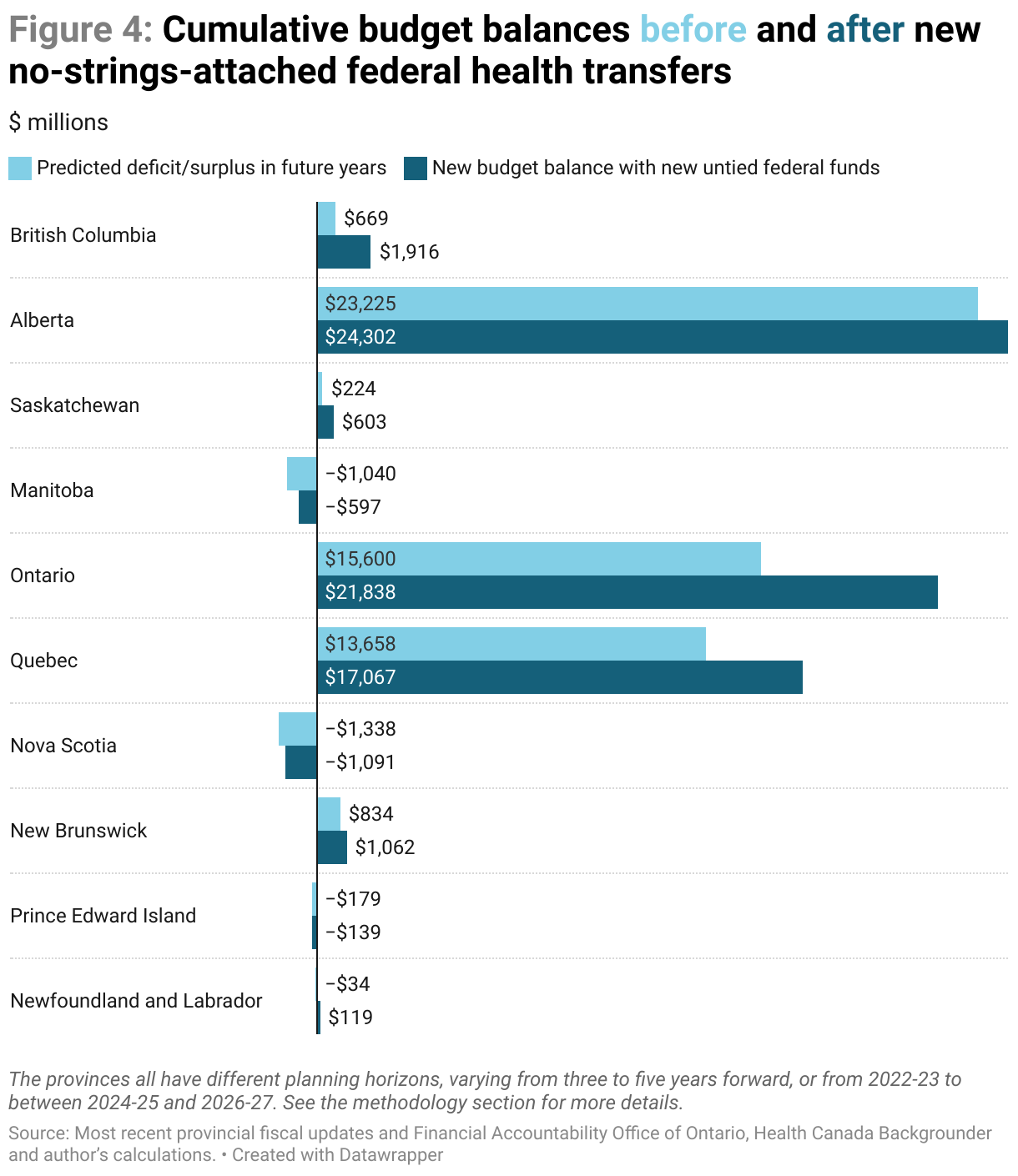
All of the big provinces—B.C., Alberta, Quebec and Ontario—have budgetary surpluses rolling in. If they wanted to fix health care today—and it is a provincial responsibility—they don’t have to ask permission, they can just snap their fingers and do it.
Need to hire more nurses? Need to fully staff emergency rooms and expand capacity? Need to clear wait list backlogs? Money isn’t the object. Ontario is projecting $15.6 billion in surpluses over the next five years. Alberta is projecting $23.3 billion in surpluses over the next three. Quebec is projecting $13.7 billion in surpluses in the next five.
This is without additional federal transfers to those provinces.
Remember, just under half of new federal transfers aren’t required to be spent on health care. It’s just new revenue. Back in 2021, the provinces said they’d spend it all paying down their deficits. But now those deficits are massive surpluses.
So those new no-strings-attached “health care” transfers will just make massive surpluses even more massive. For instance, the Financial Accountability Office of Ontario is projecting a total of $15.6 billion in surpluses over the next five years—new no-strings-attached health care money would kick that up to $21.8 billion. Quebec, would move from $13.7 billion in surpluses over the next five years to $17.1 billion.
Conclusion
Budget surpluses may be on the horizon, but the provinces are highly unlikely to sit on those surpluses. Unless considerable public pressure comes to bear, Canadians could possibly expect much of the federal health care money to be given away in the form of tax cuts. In the last round of health care accords, premiers barely waited for the ink to dry before turning that money into tax cuts.
And guess what tax cuts have never been able to accomplish in the decades that politicians have been delivering them? Better health care.
Methodological notes
The federal backgrounder didn’t break down personal support workers wage support by province. I’ve allocated it provincially based on the breakdown of the Essential Worker Wage Top-up program from the pandemic.
The cumulative budget balances in Figure 5 are over the entire available horizon for each province. Provincial contingency funds have been removed for a fairer comparison. The addition of new un-tied federal health care dollars is adjusted for each province’s time frame. For example, P.E.I has budget projections out three years: 2022-23, 2023-24 and 2024-25. Those are summed to provide the first amount in Figure 5. The additional federal amounts are the amounts expected only over those three years and only for the portion of the federal money that is untied.
The projection horizons for each province are as follows:
- Newfoundland and Labrador projects four years out
- P.E.I. projects three years out
- New Brunswick projects three years out
- Nova Scotia projects four years out
- Quebec projects five years out
- Ontario projects five years out
- Manitoba projects four years out
- Saskatchewan projects four years out
- Alberta projects three years out
- B.C. projects three years out
The following is the underlying estimates behind Figure 2.
Notes
- While much of the new federal money is allocated roughly by population, the bilateral agreements are not. They provide lower amounts to Quebec and Ontario than their populations would suggest. It’s unclear why this was done, but it’s the reason why the ratio of the money transfers to actual health care expenditures is lower for these two provinces.
- If you calculate the annual change in provincial consolidated revenue between the status quo (Table 4) and CHT increase (Table 6) scenarios from 2021-22 through 2030-31.
- Operating expenditures exclude debt-servicing charges. I’m excluding debt charges because the Annexes of the paper calculate the impact of changing debt loads on provincial expenditures via debt servicing costs. The argument being made is that by shifting projected debt from the provinces to the federal government, which pays a lower interest rate, the system as a whole can save money.

