
Many countries face the challenge of rising medical care costs, stretching government budgets and creating pressures on other spending priorities. These growing medical costs might be considered reasonable if more medical spending was the best way to improve health outcomes. But this is not the case, as revealed by evidence from many jurisdictions, including Canada.
Even as medical expenditures grow, the potential of social spending to improve population health has remained largely unexplored. Although health professionals acknowledge the pivotal role of social, economic, and environmental factors in shaping health outcomes, policy reforms in Canada have often favoured medical spending, sidelining the significance of social policy domains, including income support, housing, child care, and other policy targets.
Exploring the intricate interplay between social expenditures, medical expenditures, and common health outcomes offers valuable insights for optimizing resource allocation and improving population health.
Unlocking the ratio’s potential
A series of studies spanning Canada, the United States, and other developed nations have cast the spotlight on a compelling metric—the ratio of social expenditures to expenditures on medical care—and its profound link to health outcomes.
This ratio is a gauge of relative investments in the building blocks for a healthy society compared to investments in treating illness and injury. By consolidating two distinct expenditure categories into a single value, this ratio facilitates analysis and monitoring of the balance of expenditures between these different priorities, as well as cross-regional and cross-country comparisons, presenting a clear picture of resource allocation trends.
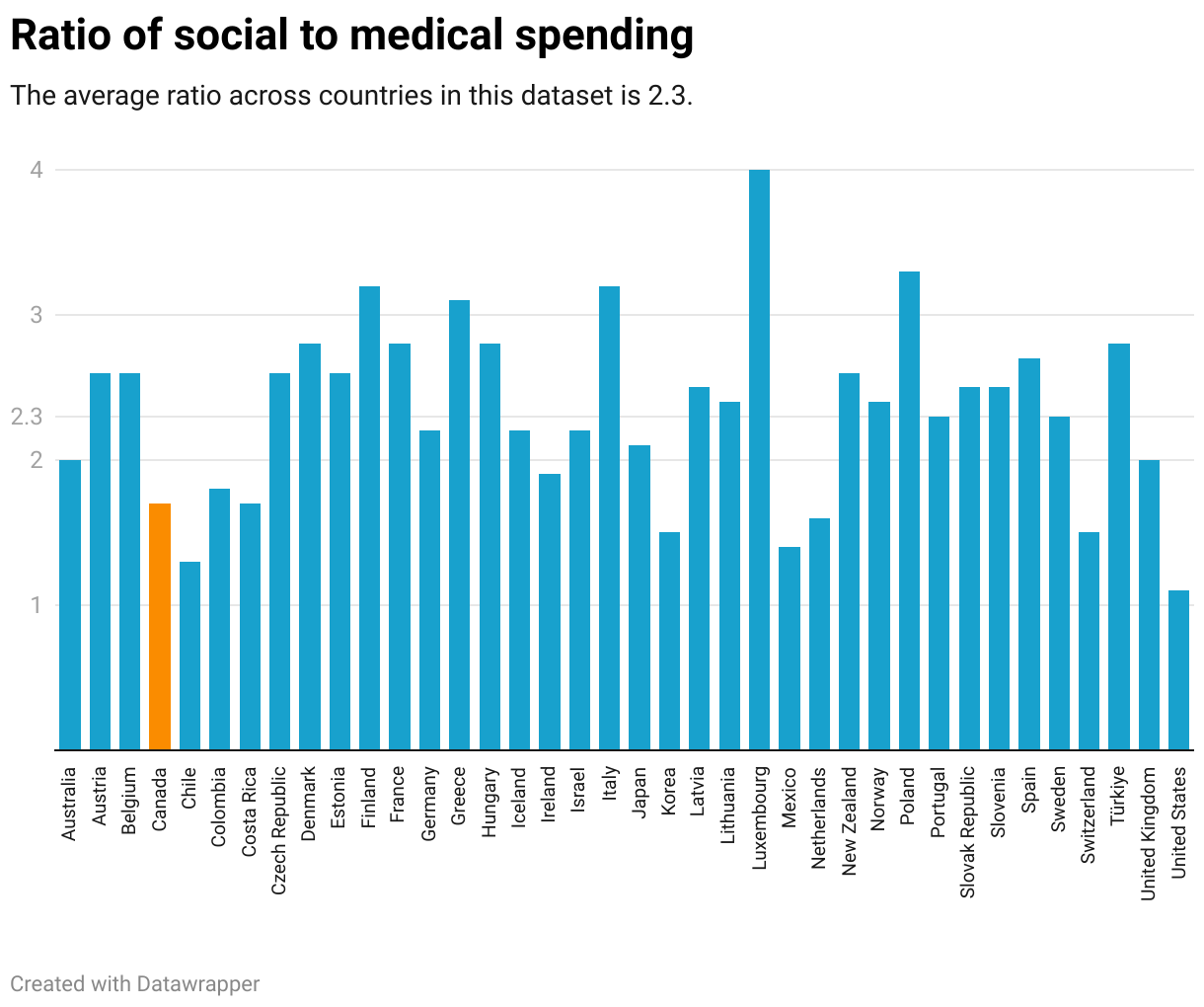
To better visualize this concept, the following graph illustrates the social expenditure-to-medical expenditure ratio across different countries from 2019. The x-axis represents countries, while the y-axis represents the ratio values. This graph offers an overview of how different nations allocate their resources between social expenditures and medical care, providing insights into potential correlations with health outcomes.
Most significantly, studies on the ratio consistently highlight the positive consequences of directing a larger proportion of governmental spending toward social services compared to medical care.
Summary of the evidence
Led by Daniel Dutton of Dalhousie University, multiple Canadian studies point to the positive health outcomes that emerge when government budgets grow social spending more urgently than medical spending.
A study using provincial expenditure data from 1981 to 2011 found that when provinces increased social spending relative to health spending, they were more likely to reduce potentially avoidable deaths and increase life expectancy.
Data from a second study of nine Canadian provinces from 1981 to 2017 affirmed that a higher ratio of social-to-medical spending was a predictor of improved health outcomes, particularly within regions facing income inequality.
A third study of budget expenditures in eight provinces between 1992 and 2018 shows that an increasing social-to-medical spending ratio is associated with lower levels of colorectal, breast and prostate cancers—but did not find a relationship between the ratio and lung cancer.
These Canadian data are consistent with international evidence. International studies, many led or motivated by the work of Elizabeth Bradley at Yale University, reveal that OECD countries and U.S. states that prioritized higher ratios of social-to-medical spending achieved a more favorable spectrum of health outcomes when contrasted with jurisdictions exhibiting lower ratios. Infant mortality decreased, life expectancy increased, and potential life years lost decreased significantly in jurisdictions where the ratio of social spending was higher.
Similarly, research led by Daniel Park, at the University of Manitoba, found higher ratios of social-to-medical care spending correlate with a decline in deaths related to mental health issues across developed countries.
Beyond the ratio
Findings from studies on the ratio of social-to-medical investments confirm what other research consistently shows: the importance of social spending in improving population health.
In Canada, investing in health, social services, and education affects the overall health of the population by reducing mortality rates.
European research highlights how social protection spending has a bigger impact on life expectancy at birth than medical care spending, and that investing in public health and social services can improve life expectancy and lower infant mortality rates.
In the United States, the ratio findings align with evidence that jurisdictions that allocate greater proportions of their medical expenditures to community health care, public health, and related domains experienced improved health outcomes.
Prioritization of clinical medical care spending in California also has been shown to lead to diminished investments in public health and social initiatives, potentially compromising health outcomes within that state.
Navigating ahead
The ratio is a valuable tool because it distills complex data and intricate relationships into a single, simple, accessible measure for governments to report and stakeholders to monitor. In a world in which governments grapple with financial constraints, the ratio emerges as a concise summary tool that comprehensively signals the degree to which decision-makers are aligning their budget allocations with health science conclusions about the optimal balance between investments in the building blocks for a healthy society compared to funding for medical care after people fall sick or injured.
By presenting a clear comparison between social and medical spending—flip sides of the same health coin—the ratio empowers policy-makers to make better decisions about health and well-being in a context in which resources are limited, demands are high, and demographics are changing.
The ratio offers a key performance indicator for the evaluation of resource distribution and its potential impact on population health.
Policy-makers can use the ratio to identify health gaps within their population in order to optimize health outcomes for all, investing wisely in well-being from the early years onwards.
Guided by cross-country comparisons, policy-makers can also use the ratio to identify variation between their jurisdiction and others in search of data-driven benchmarks for budget allocations between medical and non-medical departments that will yield the greatest chance of improving population well-being.

